Table of contents
Understanding the menstrual cycle hormonally is often not easy, as it doesn't always follow the „rules“ and sometimes does whatever it wants.
Female hormone metabolism is a complex and highly sensitive system in which multiple organs, such as the ovaries, adrenal glands, uterus, and pancreas, collaborate in a finely tuned hormonal feedback loop. A deeper understanding of these processes is crucial for correctly interpreting symptoms and taking targeted action.
The endocrine system
The adrenal gland, ovaries, pancreas, and gastrointestinal tract together form a network of hormone-producing organs.
Hormones are chemical messengers and are part of the complex hormonal feedback loop. These hormones constantly transmit information, telling organs what to produce and regulating numerous processes that are essential for our well-being.
If we exclusively focus on a single symptom or treat a single hormone without considering the others, we can easily overlook the actual cause. For example, if the adrenal gland is under a lot of stress for years Cortisol distribute, she can't get enough Progesterone and Testosterone produce. The consequences of these defects are considerable.
The main hormones
Estrogen - The Hormone of Femininity
Estrogen is probably the best-known female hormone. It is responsible for the development of secondary sex characteristics, creates curves, and plays a deep role in our emotional and social behavior. It is the hormone of nesting, the desire to care for family, and nurturing relationships.
Differentiation
When we talk about estrogen, we're actually talking about a family of three different hormones: Estradiol, Estrone and Ostreol.
They differ fundamentally in their chemical structure, biological activity, sources in the body, and physiological functions. Understanding these differences is crucial for effective hormone therapy and for understanding why women in the Perimenopause can suffer, even if their estrogen blood tests may appear „normal.“.
Estradiol – The Power Hormone
Estradiol, chemically known as 17β-estradiol, is the most biologically active Estrogen and is therefore often referred to as the „real“ or „primary“ Estrogen designated. With a relative biological activity of 100 percent, Estradiol about twelve times stronger than Estrone and eighty times stronger than Ostreol.
It is mainly used in the Granulosa cells the Ovarian produced, especially during the Follicular phase the menstrual cycle, when the Estrogen-concentration continuously rises, to trigger ovulation. During the Luteal phase remains the Estradiol-Concentration increased, but not as dramatically as with preovulatory Peak.
The functions of Estradiol are diverse and vital. It is the hormone responsible for the buildup and proliferation of the uterine lining, a process necessary for the implantation of a fertilized egg. Estradiol also regulates bone metabolism by activating Osteoblasts (bone-forming cells) and inhibition of Osteoclasts (bone-resorbing cells), thereby maintaining stable bone density. This is particularly important for the prevention of Osteoporosis, a major problem for post-menopausal women.
Cardiovascularly impacts Estradiol protective by dilating blood vessels, improving endothelial function, and thereby lowering blood pressure and the Cholesterol metabolism improved. In the brain, it plays Estradiol a crucial role in cognition, memory, and neuroplasticity, the brain's ability to form new neural pathways. It promotes Serotonin Production, which is important for mood regulation. Also sexual function and Lubrication are strong of Estradiol dependent.
In the menstrual cycle, after Estradiol a characteristic pattern: low during menstruation (10-20 pg/mL), then rising during the Follicular phase and reaches a peak of 200-400 pg/mL just before ovulation, and then remains during the Luteal phase elevated at a moderate level (100-150 pg/mL).
With the start of the Perimenopause will this pattern become chaotic, because the Estradiol-Values can fluctuate wildly, sometimes extremely high, sometimes unexpectedly low. After the Menopause sink Estradiol-Spiegel dramatisch unter 20 pg/mL fallen und dort bleiben.
Estrone – Backup Hormone
Estrone, chemically very similar to estradiol, but with only a slightly different structure. It is about twelve times weaker Estradiol. Despite this lower potency, it plays Estrone a modest role during the reproductive years, but becomes increasingly significant during menopause.
Unlike Estradiol, which is mainly from the Ovarian is produced, arises Estrone primarily through peripheral conversion of Androstenedione, a precursor from the adrenal glands, mainly in adipose tissue, skin, and liver.
This is why overweight women tend to have higher Estrone-Have mirrors, especially after the Menopause.
During the reproductive years, Estrone only about fifteen to twenty percent to the total estrogenicity. Its biological effect is much weaker. It is less effective in proliferation of the endometrium, less effective for bone density, cardiovascular, and neurological protective effects than Estradiol.
However, estrone retains some basic estrogenic effects, and its role becomes increasingly important with age.
After menopause, a dramatic shift occurs: the ovaries hardly produce any Estrogen, but adipose tissue continues to Estrone free.
In many postmenopausal women, Estrone actually the main source of estrogen effects in the body. This has both positive and negative consequences.
The positive is that women with increased body weight after menopause may have better bone density values, a phenomenon called „fat protects bones.“.
The negative, however, is that Estrone continuously and cyclically. Unlike Estradiol, which breaks down during menstruation (giving the cells a „rest phase“), the body is constantly Estrone exposed to continuous proliferative stimulation.
This is associated with an increased risk of breast and endometrial cancer, which is one reason why overweight postmenopausal women have increased cancer risks.
The cycle pattern of Estrone is much more stable than that of Estradiol, with only slight fluctuations throughout the menstrual cycle. This is because it originates from peripheral tissues, which are not cyclically regulated like the ovaries.
Estriol – Pregnancy Hormone
Ostreol it's the weakest of the three Estrogens, about eighty times weaker than Estradiol and six times weaker than Estrone.
Its chemical structure differs by an additional Hydroxyl-group that it creates during body metabolism.
The key to understanding Ostreol lies, however, not in its weak potency in the non-pregnant state, but in its massive significance during pregnancy.
Outside of pregnancy Ostreol practically undetectable in a woman's blood and has no clinical significance. A blood test for Ostreol would be pointless in a non-pregnant woman.
However, the situation changes radically during pregnancy. Ostreol is primarily produced by the fetal liver and placenta, not by the mother.
Its production is directly dependent on fetal activity and fetal well-being. This makes Ostreol into a valuable monitoring marker during pregnancy.
The function of Ostreol During pregnancy, it specializes in vasodilation in the Placenta, improves blood flow, enabling better nutrient absorption for the fetus.
It contributes to the preparation of the uterus for childbirth by increasing the elasticity of the Myometrium (Uterine muscle) increased.
Interestingly, Ostreol less strongly proliferative for the Endometrium as Estradiol, pregnancy is not the time for Endometrium-Growth (endometrial lining), which suggests why pregnant women do not have the same risk of endometrial cancer as women with chronically elevated Estrone.
Ostreol plays an important role in fetal immune tolerance, it helps the maternal immune system not to reject the genetically „foreign“ fetus.
The Estriol-Speculum levels rise continuously during pregnancy: from practically zero at week 8, to about 5 ng/mL at week 20, to about 20 ng/mL at week 30, and finally to 30-50 ng/mL at week 40 – a massive increase. After birth, estriol levels quickly drop back to undetectable levels as the placenta is removed.
Clinically Ostreol used as part of the triple screening in pregnancy between the 16th and 18th week of gestation. A low estriol level can indicate a chromosomal disorder like Down syndrome. However, a low estriol level is not definitive; many women with low levels give birth to perfectly healthy babies. It is a screening tool, not a diagnostic tool, and is not covered by health insurance. Instead, it is considered an "IGeL" service and must be paid for privately.
The following values are determined from prenatal blood:
- Alpha-Fetoprotein (AFP)
- free beta-hCG (human chorionic gonadotropin)
- unconjugated estriol (uE3)
These values will be together with the maternal age, dem Gestational age and other factors such as weight and medical history are used to determine the Risk of chromosomal abnormalities to calculate for the unborn child. This primarily includes:
- Down Syndrome (Trisomy 21) – Recognition rate approx. 74 %
occurs in 1 in 600 live births; is not a disease, but rather an immutable genetic anomaly that affects physical and mental development and is based on a random misdistribution of chromosomes during oocyte formation. - Edwards Syndrome (Trisomy 18) – Recognition rate approx. 70 %
occurs in 1 in 5,500 live births and leads to severe developmental disorders and numerous malformations; treatment is symptomatic and aimed at relieving discomfort.
Half of the newborns die within six days, only 5 to 10 percent survive a year, and about 15 percent reach the age of five. - Neural tube defects (Non-Invasive Prenatal Testing, e.g., Spina Bifida) – Detection rate approx. 80 %
occur in 1 to 1.5 of 1,000 live births. Congenital malformations of the central nervous system that result from incomplete closure of the neural tube during early embryonic development, most commonly between 22 and 28 days after conception.
The neural tube develops from the neural plate and later forms the brain, spinal cord, spine, and skull. In a neural tube defect, the closure does not occur, which can result in open or closed malformations.
Comparison and Clinical Implications
The three Estrogens can be considered specialized tools, each performing a different task.
Estradiol the main player during reproductive years, responsible for mucosal buildup, bone density, cardiovascular protection, and neurological function.
Estrone is the weak backup system, which plays only a minor role during the reproductive years, but becomes the main source after menopause, with all the associated positive and negative consequences.
Ostreol is a highly specialized hormone that is mainly relevant during pregnancy.
Understanding these differences is crucial to understanding why blood tests can sometimes be confusing.
A woman in the Perimenopause could normal or even high Total estrogen-To have mirrors, but if these are primarily made of Estrone exist (due to anovulation and peripherally increased conversion), while the biologically more active Estradiol is low, it will nevertheless have the symptoms of a Estrogen- to experience deficiency. She will complain of hot flashes, headaches, bone pain, and memory loss, not because she lacks Estrogen hat, sondern weil sie nicht das richtige Estrogen has.
In the Perimenopause is a common situation that women with anovulatory cycles have a relatively normal or even high Estrone- Have mirror, but a low Estradiol-mirror, because there is no ovulation and therefore no large ovarian-produced amount of Estradiol. This explains why women can suffer during this phase despite „normal“ estrogen levels.
Therapeutically, this has implications. If hormone replacement therapy is necessary, it is typically Estradiol used, not Estrone, because estradiol is the biologically active hormone that offers the most protection.
Some traditional HRT preparations contain conjugated Estrogens, that a mixture of Estradiol, Estrone and Ostreol are, although Ostreol is useless in non-pregnant women, its presence in traditional preparations is a historical accident, not a therapeutic reason.
Diagnostically, this means that if a hormone deficiency or imbalance is suspected, one should not simply„Estrogen“should be measured, but specifically Estradiol, Estrone and Progesterone in the right cycle phases.
A single test is often not sufficient; multiple tests over several cycles may be necessary to understand the pattern. A woman's symptoms are often more reliable than a single blood test, especially in the Perimenopause, when the hormones are chaotic.
Functions of Estrogen
- Mucosal health
Moist mucous membranes in the mouth, eyes, and vagina - Bone stability
Calcium deposition and bone density - Cardiovascular
Vascular elasticity and blood pressure regulation - Emotional well-being
Mood, motivation, and sensuality
Estrogen is primarily produced in the first half of the menstrual cycle. Its role begins immediately after menstruation: it stimulates the uterus to build up its lining, similar to laying down cotton wool, ready to gently receive a fertilized egg.
When the woman gets older and into Premenopause entry, begins Estrogen to sink. This leads to numerous symptoms that are often overlooked as the cause:
- Headache
- sleep disorders
- irritability
- Hot flashes
...the general feeling that the body is „falling apart.“.
Key takeaway
Many women report high blood pressure or shoulder painFrozen Shoulderthat are related to estrogen deficiency.
A low-floor EstrogenArteries can contribute to high blood pressure because the vessels lose their elasticity. Shoulder pain occurs because many Estrogen receptors available, and without sufficient Estrogen these joints and muscles can suffer.
Progesterone - The Hormone of Tranquility
While Estrogen the hormone of the first half of the cycle is, is Progesterone the hormone of the second half. After ovulation (which occurs in the middle of the cycle), Progesterone released from the corpus luteum, the remnant of the follicle after ovulation.
Progesterone tells the uterus that enough lining has been built up, and prepares it to receive a fertilized egg.
Progesterone is the hormone that calms, helps with sleep, and regulates nerve excitability. Women suffering from progesterone deficiency often report feeling „constantly tense,“ that small things irritate them, and that they can no longer sleep in the second half of their cycle.
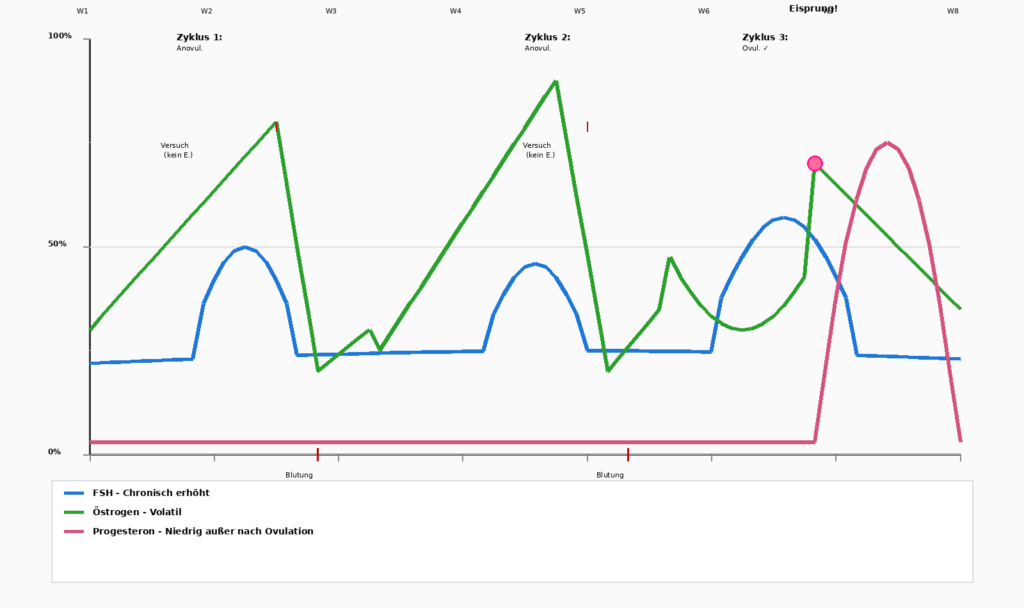
Progesterone is often the first hormone to be produced in lower amounts. A woman can still have her period for years but not ovulate properly, meaning she has little or no Progesterone produces more.
In such cases, the uterine lining can grow uncontrollably, leading to extreme bleeding that confuses the woman because she doesn't understand why the amount is so massive.
Signs of progesterone deficiency
If a woman under
- Extreme insomnia
- strong irritability
- severe menstrual cramps
- uncontrolled mood swings
- unexplained anxiety disorders
suffers, especially if these symptoms are new or have worsened, progesterone deficiency is often the trigger.
Paradoxically, doctors often fail to recognize this because they focus on the regular menstrual cycle, not on the lack of ovulation.
Testosterone - Energy and Strength
Although Testosterone often perceived as the „male hormone,“ women also produce Testosterone. There is energy that helps build muscle, improves metabolism, and contributes to libido.
Sufficient testosterone is associated with vitality and the feeling of being able to „keep going.“.
When a woman has too low a testosterone level, she often feels tired and low on energy. The problem is exacerbated when chronic stress overloads the adrenal glands: Then the adrenal glands cannot produce enough testosterone to compensate for the deficit from the ovaries.
Cortisol – The Survival Hormone
Cortisol is the stress hormone released by the adrenal gland. In moments of great stress Cortisol activates the „fight or flight“ mode, helping to overcome crises.
The problem arises when Cortisol remains chronically elevated:
- persistently high blood sugar
- raises blood pressure
- „steals“ resources from the adrenal gland for the production of Progesterone and Testosterone missing
This creates a vicious cycle:
Chronic stress → high Cortisol too little Progesterone and Testosterone → lower stress resilience → even higher Cortisol.
The woman feels trapped, exhausted, and cannot escape the spiral.
Do estrogen and stress cause lipedema?
The question of the causes of lipedema is one of the central questions for affected women and doctors. For decades, this disease was overlooked or explained by a lack of willpower, with the advice: „You just need to lose weight!“
Today it is known that lipedema is a biological disease in which genetic predisposition and hormonal factors interact. Both Estrogen as well as stress seem to play an important role in the onset and worsening of this condition.
Basics of Genetics and Hormone Triggers
Lipedema is a chronic disorder of the subcutaneous adipose tissue, characterized by abnormal proliferation and pathological accumulation of fat cells, typically in the legs or sometimes in the arms. The buttocks and upper body are usually unaffected, leading to a characteristic ratio: a slender torso but voluminous legs. The disorder affects women in over 95 percent of cases, strongly suggesting a hormonal component.
Understanding the causes of lipedema requires distinguishing between two different biological levels: genetic predisposition and hormonal triggers.
An important finding from modern research is that genetic predisposition alone is not sufficient to trigger lipedema; it requires a trigger.
Studies show that up to 60 percent of affected women have relatives with the same symptoms, indicating a strong hereditary component. However, not all genetically predisposed women develop the condition; some remain symptom-free throughout their lives. This suggests that the genetic „time bomb“ needs to be triggered by external factors.
Estrogen as the primary trigger
In over 85 percent of affected women, the first outbreak of lipedema occurs during a phase of hormonal change. These are typically three life events:
- Puberty
- pregnancy
- Menopause
The fact that lipedema so consistently coincides with these hormonal transitions implies that Estrogen plays a central role.
During puberty, the Estrogen-The mirror shows a dramatic change. Around this time, many young girls notice that their legs swell abnormally and gain volume, while their upper body remains slim.
This is often overlooked at this time or misinterpreted as normal weight gain. If the girl also starts taking the birth control pill, which further increases estrogen exposure, lipedema development is often accelerated.
Doctors and patients attribute weight gain to the pill, without realizing that an underlying lipedema condition has awakened.
Even during pregnancy, massive hormonal changes occur. The body not only produces more Estrogen, but also an increased ratio of Estrogen to Progesterone. Many women with pre-existing lipedema report a significant worsening of their symptoms during pregnancy: more swelling, more pain, and faster progression of the condition. In some cases, lipedema manifests for the first time during pregnancy when the genetic predisposition was present but had not yet become apparent.
In menopause, the situation is paradoxical: The Estrogen- The scale sinks dramatically, and yet many women with lipedema can experience a worsening. This could explain that not the absolute Estrogen-level the problem is, but rather the fluctuation and the imbalance between Estrogen and other hormones such as Progesterone and Testosterone. When the body gets out of hormonal balance, whether through high or falling levels, lymphedema symptoms seem to worsen.
The biological mechanisms by which Estrogen The exact mechanisms by which lipedema affects the body are not yet fully understood, but several theories have found empirical support.
A theory states that it is about the density and function of Estrogen-Receptors It enters the subcutaneous adipose tissue. Adipose tissue in the legs may have a higher density of estrogen receptors than adipose tissue elsewhere in the body, a „local phenomenon“ rather than a systemic one. When estrogen binds to these receptors, it could trigger local signals, leading to abnormal fat cell proliferation and enlargement.
Another theory concerns capillary action: Estrogen could increase the permeability of the smallest blood vessels, leading to fluid leaking into the tissue, which is exactly what is observed in lipedema.
A particularly interesting new research finding relates to the Progesterone metabolism. Scientists have a Gene identified, for the enzyme Aldo-Keto Reductase encoded. This enzyme is responsible for progesterone metabolism.
Women with a Mutation in this gene show abnormal progesterone levels, especially in local adipose tissue.
This could be a decisive factor, not just the Estrogen-level, but also the balance between Estrogen and Progesterone in local adipose tissue could be crucial. A deficiency in progesterone or an imbalance between estrogen and progesterone could drive the pathological fat processes in lipedema.
Hormonal imbalance and lipedema flares
A common pattern observed in clinical practice is the „flare“ phenomenon in lipedema. Patients report that their lipedema symptoms do not worsen continuously but rather in episodes, with symptoms sometimes being stable and then suddenly experiencing a dramatic worsening with increased swelling, pain, and possibly even increased weight gain in the affected area.
These flare-ups often coincide with hormonal changes:
- the start or discontinuation of the Pill
- one pregnancy or Miscarriage
- Beginning of the Menopause.
The mechanics of these surges seem to be related to hormonal imbalance. When the body is put into a state where estrogen is high and progesterone is low, or when the ratios fluctuate chaotically, this appears to „trigger“ lipedema fat cells. They multiply, they enlarge, and they lead to increased symptoms.
This explains why some women experience a worsening of their lipedema while using hormonal contraception, especially estrogen-dominant contraceptives, and why perimenopause, a time of extreme hormonal fluctuation, is particularly difficult for many lipedema patients.
Therapeutically, this finding has implications. Some lipedema experts advise patients to forgo hormonal contraception or at least experiment very carefully to see if a particular contraceptive worsens their symptoms.
In some cases, it is recommended for patients wishing to conceive to undergo liposuction (therapeutic fat removal) before pregnancy to reduce the burden of lipedema before the hormonal turbulence of pregnancy occurs.
Stress, Cortisol, and Inflammation
While hormone research for lipedema has been ongoing for decades, a more recent finding is the role of psychological stress.
Current clinical observations and initial research findings suggest that stress, in addition to hormones, could be a significant trigger factor for lipedema flare-ups.
When the body is under stress, whether acute stress (like a traumatic event or a significant life event) or Chronic stress (such as work stress or family conflicts), he Cortisol free. Cortisol, the classic „stress hormone,“ is a body's own Corticosteroid, which normally mobilizes the body to deal with challenges. However, under chronic stress, cortisol levels remain permanently elevated.
Several clinical observations have shown that lymphedema patients experiencing increased psychological stress often experience lymphedema flare-ups immediately afterward.
Some patients report that after a death in the family, job loss, or a breakup, their lipedema symptoms have dramatically worsened, sometimes with a delayed reaction of weeks to a few months. This suggests a biological mechanism through which Psychological stress exacerbates lipedema pathology.
Cortisol is known as a pro-inflammatory hormone that leads to systemic inflammation when chronically elevated.
Lipidema itself is associated with chronic inflammatory processes in the affected adipose tissue, where abnormal lipidema fat cells are constantly surrounded by inflammatory mediators. An increase in the Cortisol-Mirrors could amplify this inflammation through stress.
In addition, it suppresses Cortisol under chronic elevation of the immune system, which in turn can lead to abnormal inflammation patterns.
The lymphatic function, which is often impaired in lipedema, could also be affected by chronic stress and increased Cortisol further hindered.
stress and Cortisol also affect the hormone axis itself. Chronic stress can lead to Dysregulation of the Hypothalamic-Pituitary-Ovarian Axis lead, which in turn leads to abnormal estrogen and progesterone patterns leads.
Stress could either directly (through Cortisol worsen lipedema.
Genetics, Hormones, Stress as a Whole Picture
The current understanding of lipedema has evolved from a simple „weight problem“ explanation to a complex model where multiple factors interlock.
The best current phrasing is: Genetic predisposition is necessary but not sufficient. A trigger factor, usually several factors, is needed for lipedema to manifest.
The primary triggers are hormonal in nature:
- Puberty
- Start of hormonal contraception
- Pregnancy,
- Perimenopause
- Menopause
These are the critical points where many women with a genetic predisposition first notice their lipedema.
However, secondary factors also play a role. Chronic psychological stress can trigger or worsen lipedema, likely through a combination of increased cortisol, inflammation activation, and secondary hormone amplification. Being overweight is not a causal factor, but it can worsen the symptoms.
An overweight woman without a genetic predisposition to lipedema will never develop lipedema, but a genetically predisposed woman can worsen her symptoms due to being overweight.
This complexity also explains why lipedema is so variable. Two women with identical genetic predispositions can have completely different courses, depending on the hormonal triggers they experience and the stress they are exposed to.
A woman might go through puberty with minimal symptoms and then experience a pregnancy that leads to a dramatic lipedema flare-up.
Another woman might be minimally affected her whole life, until menopause confronts her with a new surge.
Clinical implications
Understanding that estrogen and stress are relevant factors has therapeutic implications:
- Lipedema patients should be very careful when choosing contraceptives. Switching to a low-dose estrogen product or non-hormonal contraceptive methods could improve symptoms in some cases.
- Stress management is not only important for psychological well-being but also has a direct medical component: chronic elevated stress can actually worsen lipedema and should be actively addressed.
- Diagnostic skepticism is warranted when a blood test shows „normal“ estrogen levels, but a patient is suffering from lipedema flare-ups. The problem may not lie in the absolute estrogen level, but in the Balance between estrogen, progesterone, and testosterone, or in the local hormone concentrations in the adipose tissue itself, which are not detected by a blood test.
An experienced lymphedema doctor will do more than just read the blood test; they will ask the patient about stress, life changes, and menstrual patterns. - Therapeutic that there are other avenues beyond liposuction and compression therapy. Stress relief, Stress management techniques, possibly even Specific dietary adjustments, that the Stabilize hormone balance, could theoretically improve lipedema behavior. This is currently being actively investigated.
Studies
Estrogen
- FANG et al. (2026) - Impact of hormones on lipedema development: a systematic literature review„
„Lipedema appears to be a multifactorial disease primarily caused by hormonal dysregulation - particularly related to estrogen - as well as metabolic and possible genetic components. The findings support the reclassification of lipedema as a hormonally influenced disease distinct from obesity and underscore the need for further research into diagnostic biomarkers, targeted therapies, and the role of genetic predisposition.“ - VIANA et al. (07.2025) - „Menopause as a Critical Turning Point in Lipedema“„
- KATZER et al. (2021) - „Lipedema and the Potential Role of Estrogen in Excessive Adipose Tissue Accumulation„
Shows that estrogen promotes adipogenesis through ERα activation and PPARγ expression upregulation - VIANA et al. (07.2025) - „Menopause-induced estrogen deficiency amplifies adipose tissue dysfunction by suppressing ERα signaling, enhancing ERβ activity, and disrupting mitochondrial function.„
„The systemic decline of circulating estradiol, coupled with enhanced intracrine estradiol production in affected adipose tissue, driven by aromatase and 17β-HSD1 overexpression and 17β-HSD2 deficiency, along with an imbalance favoring ERβ over ERα signaling, creates a pro-inflammatory, pro-fibrotic, and estrogen-dominant microenvironment. This hormonal milieu promotes adipocyte hypertrophy, chronic inflammation, extracellular matrix remodeling, and resistance to lipid mobilization.“ - CIFARELLI et al. (2025) - „Lipedema: From Women’s Hormonal Changes to Nutritional Intervention„
Shows chronic inflammation as a core mechanism, also mentions leaky gut, often caused by dysbiosis or other intestinal barrier disorders, and goes into more detail on anti-inflammatory measures and supplements.
„This condition leads to chronic, low-grade inflammation, partly due to the translocation of LPS (lipopolysaccharides), which are components of the outer membrane of Gram-negative bacteria, from the gut into the systemic circulation.
When LPS circulates through the bloodstream, it also reaches adipocytes, which then produce pro-inflammatory cytokines like TNF-α, IL-6, and IL-1β, altering adipocyte functions and causing a significant local inflammatory response.“
Stress and Cortisol
- DINNENDAHL ET AL. (09.05.2024) - „The Expression of Adipogenic Marker Is Significantly Increased in Estrogen-Treated Lipedema Adipocytes Differentiated from Adipose Stem Cells In Vitro„
„This study indicates that the expression of ERs and several estrogen-metabolizing enzymes differs in lipedema, suggesting estrogen may play a role in the dysregulation of adipose tissue in lipedema.“
Inflammatory biomarkers
- Laura Patton et al. – 01/27/2024 - „Observational Study on a Large Italian Population with Lipedema: Biochemical and Hormonal Profile, Anatomical and Clinical Evaluation, Self-Reported History„
Largest known cohort study with 360 women with lipedema in Italy
„Normal blood tests do not rule out lipedema“ - the problem does not lie in the systemic hormone levels, but in the local hormone metabolism in adipose tissue - Fühner R. et al. – (12/07/2022) - „Lipedema: Insights into Morphology, Pathophysiology, and Challenges„
„Lipedema can be differentiated from obesity and lymphedema based on its unique morphological and molecular characteristics.“
Multidisciplinary overview
Cifarelli V. – (2025) - „Lipedema: Progress, Challenges, and the Road Ahead„
Understanding the Menstrual Cycle
The menstrual cycle is a four-week dance between two hormones: Estrogen and Progesterone. To fully understand the effects of these hormones, it is important to divide the cycle into its phases.
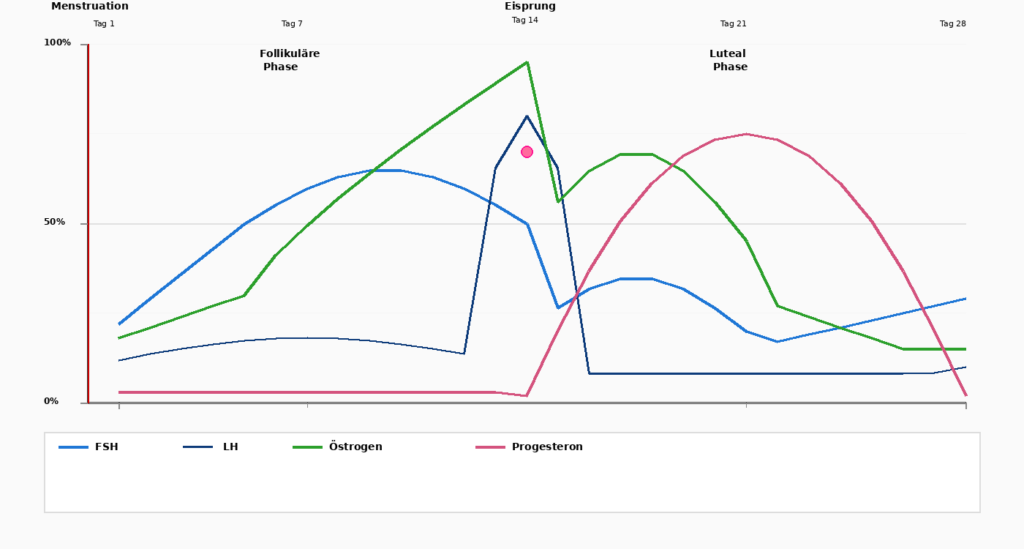
Days 1–5
Menstruation
The cycle begins with menstruation, when the built-up uterine lining is shed. Estrogen and Progesterone are at their lowest values.
Days 1-14
Follicular phase
After menstruation, the Pituitary gland, FSH (follicle-stimulating hormone), which stimulates egg development in the ovaries. At the same time, Estrogen to rise. The body becomes more active, energy increases, and the uterine lining begins to grow.
Day 14
Ovulation
A dramatic increase in LH (Luteinizing Hormone) triggers ovulation. The egg is released and travels into the fallopian tube. At this point it reaches Estrogen its peak, before it suddenly drops. At the same time, it begins Progesterone to climb.
Days 15-28
Luteal phase
After ovulation, it dominates Progesterone the second half of the cycle. Progesterone prepares the uterine lining in case an egg has been fertilized.
Simultaneously calms Progesterone the body: Sleep can become deeper, nervousness decreases. If the egg is not fertilized, it drops Estrogen and Progesterone at the end of this phase, clearly drops and triggers the next menstruation.
Hormonal fluctuations in the menstrual cycle
Estrogen Overload – The Subtle Imbalance
It is important to note that sometimes an imbalance, not an absolute deficiency, is the problem. When progesterone drops while estrogen remains relatively elevated, this creates „estrogen dominance“ (relative, not absolute). This leads to:
- Weight gain
Difficult weight loss despite dietary changes - Headache
Regular or increased headaches - Mood swings
Emotional lability - Chest tension
Persistent chest pain or tightness - Bloating
Increased abdominal bloating - irritability
Increased irritability - Heavy menstruation
Uncontrolled heavy bleeding
Changes – Perimenopause to Menopause
A woman's hormone status is not static. It goes through different phases, each with its own challenges.
- Fertile years (up to ~35 years)
Estrogen and Progesterone are in a stable rhythm. Ovulation is consistent, and menstruation is predictable. Most women have fewer symptoms. - Premenopause (ages 35–42)
Progesterone falls first. Estrogen remains high initially. This leads to classic PMS symptomsInsomnia, extreme irritability, heavy bleeding. Life feels „impossible.“. - Perimenopause/Menopause (42–49 years)
This is the most turbulent phase. Progesterone stays low, but Estrogen becomes volatile: it shoots up and then suddenly drops.
A woman doesn't know how she'll feel from day to day. Sometimes she has heavy bleeding, sometimes none at all. Sometimes she has energy, sometimes she feels completely exhausted.
Many women describe this phase as „nasty,“ worse than even the early menopause, because the unpredictability creates a feeling of no longer being in control of „it.“.
Measures for Hormonal Imbalances and PMS
The good news is that much can be done to alleviate hormonal symptoms and improve quality of life. However, the approach should be multifaceted.
Diagnostic Fundamentals
The first step is understanding your own hormone profile through testing.
Blood tests can measure levels of estrogen, progesterone, FSH, LH, and other hormones.
Saliva tests are less invasive and can also be informative.
The most important thing is not to perform these tests on random days; timing is crucial: progesterone should be at its Luteal phase preferably tested on day 21, not on the follicular Phase.
Nutrition
Modern diets are too often insufficient. Studies show that fruits and vegetables today contain about 80% fewer vitamins than 50 years ago. This is not a failure of farmers, but the result of, for example, overly intensive agriculture, depleted soils, low varietal diversity, incorrect harvesting times, and longer transport routes. Therefore, it is essential to consciously pay attention to adequate nutrient intake.
Blood sugar stability
A key to hormone health is stabilizing the Blood sugar. Women should have regular meals with sufficient protein eat. Especially in the Luteal phase (second half of the cycle) the body needs more calories and nutrients.
Stress management and lifestyle
Chronic stress is one of the main drivers of hormonal imbalances.
When a woman is under continuous stress, the adrenal gland continuously releases Cortisol ab. This competes for resources with Progesterone and Testosterone.
The solution is not, „Cortisol to lower“ (which would be impossible and dangerous during stress), but rather to reduce the sources of stress. This can mean letting go of some (partly supposed) obligations, setting boundaries, or even rethinking one's career.
Sleep
Seven to nine hours of quality sleep aren't a luxury; they're essential for hormone production and regulation. A lack of sleep intensifies Progesterone deficiency exponentially.
Dietary supplements
While good nutrition is the foundation, strategically used supplements can support the body. The key is understanding: supplements do not replace nutrition, but they fill the gaps left by modern agriculture and lifestyle.
The Magnesium Vitamin D3 Vitamin K2 Complex
These three substances are inextricably linked. However, they are often erroneously viewed in isolation from each other.
The connection:
- magnesium influences over 400 bodily processes
- Vitamin D3 (which is technically a hormone, not a vitamin) promotes calcium absorption
- Vitamin K2 activates osteocalcin, the protein that initiates calcium into the bone matrix
If any one of these three is missing or even insufficiently present, the system will not function properly.
Other essential nutrients
- Omega-3 fatty acids
Hormone regulation, cardiovascular health, anti-inflammation, vision - B Vitamins
Support of hormone metabolism and the nervous system - Vitamin C and E
Antioxidant protection, collagen formation - Zinc
Immune function and hormone production - iron
Especially important for menstruating women due to natural blood loss - Probiotics
Gut health, hormone metabolism, nutrient absorption
The gut is an often overlooked hormonal organ. A large part of hormone metabolism takes place in the gut. A healthy microbiome not only promotes nutrient absorption but also hormone recirculation. Probiotics (in special encapsulation to withstand stomach acid) can restore gut balance.
Essential oils
Essential oils are concentrated plant substances that can interact with the nervous system through inhalation and topical application. They are not a substitute for medical treatment, but a valuable addition.
Lavender – for calming
Performance characteristics
Blood pressure regulation, heart rate stabilization, muscle spasm relief, sedation
Indications
Insomnia, menstrual cramps, high blood pressure, PMS-associated symptoms
Application
3–4 drops with a carrier oil (coconut, jojoba) on the abdomen, neck, or soles of the feet. Can also be used in a diffuser.
Ylang-Ylang – Blood Pressure and Libido Regulator
Performance characteristics
Blood pressure regulation, libido enhancement, emotional balance, hormone modulation
Special feature
This oil has proven to be particularly effective against high blood pressure, even in cases where medication was not enough.
Application
2 drops sublingually (on the tongue), or topically on pulse points and neck
Magnolia -- Adrenal Adaptogen
Performance characteristics
Adrenal Support, Stress Relief, Anxiety Reduction, Panic Attack Relief
Application
Apply to the kidney area (lower back) in the morning and evening with a carrier oil. Regular use for one month shows significant effects.
Balance - Harmonization and Hot Flush
Performance characteristics
Emotional stabilization, mood balancing, hot flash relief
Application
4 drops with carrier oil on both soles of the feet in the morning after waking up.
Serenity – (Night) Relaxation
Performance characteristics
Deep relaxation, sleep promotion, mental and emotional calming
Routine
3–4 drops with carrier oil on the feet before bed leads to restful sleep.
Vetiver and Adaptive
Vetiver brings energy and vitality. Adaptive is unique, containing rosemary (for mental clarity) mixed with sedating components.
Important
Essential oils should always be diluted with a carrier oil. The dosage is individual; some women react to 2 drops, while others need 4 or more.
An Integrative Approach to Hormone Health
The key to improved hormone health lies in an integrative approach:
- Tests
Know your hormone levels, don't guess - Nutrition
Real food, regularly, with enough protein and stable blood sugar - Reduce stress
Identify and systematically reduce chronic stress - Optimize sleep
7-9 hours consistently, at the same time - Dietary supplement
Targeted, based on tests and symptoms - Aromatherapy
Essential Oils for Emotional and Physical Support - Tracking
Document symptoms, check hormone levels regularly
The goal isn't simply to alleviate symptoms, even though that's important. The goal is to support a woman so she can remain vital and vibrant through her 80s and 90s. Without this integrative approach, many women may feel like their lives are over at 50 or 60. With it, they can blossom again.
Laying a foundation isn't complicated; it simply requires clarity about what the body needs and the determination to provide it. Two minutes a day to strengthen health influences every subsequent decision made that day.