Table of contents
Burnout and Support with Essential Oils
What is burnout?
Burnout is not a sign of weakness, it is the physical and mental reaction to persistent, chronic stress that one cannot escape. The term comes from English and literally means “to be burned out.”.
The image behind it: Imagine a candle burning at both ends. Eventually, the wax runs out, and the candle goes out. Similarly, the body and mind become exhausted when too many demands are placed on too little recovery for too long.
Burnout is a state of emotional, physical, and mental exhaustion caused by excessive and prolonged stress. It occurs when you feel overwhelmed, emotionally drained, and unable to meet constant demands. As pressure mounts, you begin to lose interest and motivation in the activities you once enjoyed.
The stress system is going haywire: Our body has a built-in alarm system, the so-called HPA axis (Hypothalamus-Pituitary-Adrenal axis). During stress, it releases the hormone Cortisol Cortisol, the “stress hormone.” Cortisol is useful in the short term: it mobilizes energy, sharpens attention, and suppresses inflammation.
However, with chronic stress, something dangerous happens: the system runs at full throttle continuously. Initially, the cortisol level is permanently elevated (red alert), and later the system breaks down, with the cortisol level dropping to abnormally low values (total exhaustion). This is the classic burnout state.
What that does to the body: - Sleep disturbances (difficulty falling asleep and staying asleep) - Chronic fatigue that is not improved by sleep - Concentration problems, memory loss (“brain fog”) - Emotional numbness or irritability - Physical complaints: headaches, back pain, rapid heartbeat - Weakened immune system (frequent colds) - Digestive problems
How common is burnout? In Germany, approximately 23% of adults report symptoms of burnout. Those particularly affected include healthcare workers, teachers, managers, and the self-employed. Burnout is the most common cause of long-term disability.
How is burnout typically treated?
Burnout is officially not a standalone diagnosis in the psychiatric sense, but is often treated as exhaustion depression or an adjustment disorder.
Drug treatment
Antidepressants (SSRIs/SNRIs) – Used when burnout has developed into clinical depression – Examples: Sertraline, Escitalopram, Venlafaxine – Affect serotonin and norepinephrine – Take 2–4 weeks to become effective – Side effects: nausea, sleep disturbances, sexual dysfunction
Benzodiazepine (sedative) – Only short-term for acute panic or insomnia – Examples: Lorazepam, Diazepam – Caution: Risk of addiction with prolonged use!
Beta-blocker – Against physical stress symptoms (racing heart, trembling) – No direct effect on the causes of burnout
Important: None of these medications treat the cause of burnout; they alleviate symptoms. The actual therapy consists of behavioral changes, psychotherapy, stress management, and recovery.
Essential oils for burnout – how can they help?
Essential oils can calm the stress system in several ways:
- Directly about the sense of smell: Fragrance molecules activate the limbic system, the brain's emotional center, and can induce relaxation within seconds.
- About the nervous system: Some terpenes activate the parasympathetic nervous system (“rest and digest”) and slow down the sympathetic nervous system (“fight or flight”).
- About neurotransmitter systems: Certain terpenes influence GABA (calming), serotonin (mood-lifting), and cortisol (stress-reducing).
- Systemic: With regular use, they can regulate the stress system (HPA axis) in the long term.
Which essential oils help with burnout?
Bergamot – the cortisol killer
Bergamot (Bergamot orangeis the superstar among burnout oils.
- What's inside? Limonene (30–45 %), linalyl acetate (20–30 %), linalool (10–15 %)
- The impressive numbers: In a clinical trial, bergamot aromatherapy lowered cortisol levels by 46 %, fast as strong as a medicine!
- What else it does: Increases serotonin and dopamine, activates GABA-A receptors (calming), lowers heart rate and blood pressure
- How to apply Diffuser (5 drops, 20 minutes), Inhalation, Massage (diluted)
Lavender – the relaxation icon
Lavender (Lavandula angustifolia) is the best-researched stress oil.
- What's inside? Linalool (25–45 %), linalyl acetate (25–50 %)
- What it does: Activates GABA-A receptors (same target as sedatives, but without addiction), lowers cortisol, improves sleep quality
- Studies: A meta-analysis of 15 studies confirms a significant reduction in anxiety; lavender aromatherapy improved sleep quality among nursing staff by 60%
- Special feature: The lavender oil preparation Silexan (80 mg daily as a capsule) is clinically approved as an anxiolytic.
Rosemary – for exhaustion and brain fog
Rosemary (Rosemary) has been used as a memory herb since antiquity.
- What's inside? 1,8-Cineole (Eucalyptol), Camphor, α-Pinene, Rosmarinic acid
- What it does for burnout:
- 1,8-Cineole inhibits an enzyme that breaks down the neurotransmitter acetylcholine, keeping the brain clearer and more focused. Antioxidant: Protects nerve cells from stress damage.
- Activating: Enhances alertness and cognitive performance
- Study Rosemary aromatherapy significantly improved memory performance and attention (p < 0.05).
- Tip: Rosemary in the morning (activating), lavender in the evening (calming)
Rhodiola – The Queen of Adaptogens
Rhodiola rosea (Rhodiola) is technically a plant, not an essential oil, but one of the most important adaptogens for burnout.
- What's inside? Rosavine, Salidroside
- What it does: Regulates the HPA axis directly; reduces cortisol; improves energy metabolism in exhausted cells
- Clinical trial: A daily dose of 576 mg of rhodiola significantly reduced burnout symptoms after 12 weeks: fatigue (−54 %), difficulty concentrating (−48 %), mood (+43 %)
- Comparison with Sertraline: In one study, Rhodiola was slightly less effective than sertraline, but had significantly fewer side effects.
Ylang-Ylang – the Parasympathetic Activator
Ylang-Ylang (Cananga odorata) has an intense, floral scent.
- What it does: Activates the parasympathetic nervous system (rest and digest nerve); lowers blood pressure and heart rate within minutes
- Study Ylang-ylang inhalation lowered systolic blood pressure by 11.7 mmHg and heart rate by 9 beats/minute (p < 0.05).
- Tip: Use sparingly, intense fragrance can cause headaches in some
Sandalwood - for deep sleep
Sandalwood (Santalum albumhas a warm, woody, calming scent.
- What's inside? alpha-Santalol, beta-Santalol
- What it does: Activates GABA-A receptors; promotes deep, restful sleep; anxiolytic
- Particularly suitable: For burnout with sleep disturbances as an evening routine
Cedrol (Cedarwood) – Heart Rate and Relaxation
- What it does: Activates the parasympathetic nervous system directly; lowers heart rate; promotes deep sleep
- Study Cedrol inhalation reduced heart rate by 5.8 beats per minute and respiratory rate by 5.5 breaths per minute (p < 0.05)
Practical Anti-Burnout Routine with Essential Oils
Morning Routine (Energizing + Focusing)
- 5-minute rosemary or peppermint inhalation (2 drops on a handkerchief)
- Or: Bergamot in the diffuser during breakfast
Lunch break (stress relief)
- 10-15 minute lavender or bergamot diffuser
- Short breathing exercise: inhale for 4 seconds, hold for 4, exhale for 6
Evening Routine (Winding Down + Sleep)
- Lavender, sandalwood, or cedarwood in the diffuser (30 minutes before sleep)
- Or: 2 drops of lavender on the pillow
- Relaxing bath with lavender + bergamot (5 drops each in carrier oil)
Weekly Deep Relaxation
- Aromatherapy massage with bergamot + lavender (5 drops each in 30 ml almond oil)
- Focus on shoulders, neck, soles of the feet
What really helps? - The Evidence Pyramid

Important Notes
What to consider:
- Burnout requires treatment. – seek professional help if symptoms persist
- Essential oils are a supplement – no substitute for therapy and lifestyle changes
- Address the cause – Without stress reduction, even the best oils only help in the short term
- Do not put on the skin – Always dilute with a carrier oil (2–3 parts carrier oil to 1 part essential oil)
- Bergamot – Light-sensitive, do not expose to sun after application
- Ylang-Ylang - Use sparingly, otherwise headaches are possible
The document provides a summary in three sentences. It offers a concise overview of the main points discussed. This allows for a quick understanding of the content without needing to read the full text.
Burnout occurs when chronic stress permanently overloads the body’s stress response system (HPA axis/cortisol) and ultimately leads to a breakdown. Essential oils, particularly bergamot (−46 % cortisol), lavender (GABA-A modulation), and rosemary (cognitive activation), can directly calm the stress response system, improve sleep, and promote recovery. They are a valuable complement to psychotherapy and lifestyle changes, but do not replace them.
doTERRA Essential Oils for Burnout
Recommended oil blends and application protocol
Primary products

DIY Blends
Blend 1 – “Cortisol-Reset” (Diffuser)
Target: Normalize the HPA axis, dampen stress response

Application: Morning and evening, 30 minutes each
Blend 2: “Adrenal Support” (Topical)
Target: Adrenal Support, Energy Balance

Application: Massage the kidney area (lower back) and wrists.
Blend 3 - “Energy & Focus” (Diffuser/Inhalation)
Target: Cognitive fatigue ↓, concentration ↑

Application: Use as an office diffuser during the day; inhale directly when experiencing acute fatigue.
Blend 4 – “Relaxation & Regeneration” (Bath/Massage)
Target: Parasympathetic nervous system ↑, deep relaxation, regeneration

Application: 20-30 minute warm bath, 3 times per week
Blend 5 – “Emotional Exhaustion” (Topical, Heart)
Target: Fill emotional emptiness, restore connection

Application: On the heart area (sternum) and the palms of the hands
Application Protocol - 4-Week Plan
Week 1 - Stabilization
- Mornings: Blend 3 in the diffuser (Energy & Focus)
- Lunch Blend 1 in the diffuser (Cortisol Reset)
- In the evening Serenity Blend in the diffuser
- Daily: Balance Blend topical on soles of feet
Week 2 - Regeneration
- Mornings: Blend 2 Topical (Adrenal Support)
- In the evening Blend 4 (Bad, 3× a week)
- Daily: Adaptive blend on wrists and neck
Week 3 – Construction
- Focus on Energy Blend 3 daily
- Emotional Labor Mix 5 (hearts) daily
- Optimize Sleep: Serenity Softgels (1–2 capsules)
Week 4 – Integration
- Individual Protocol based on progress
- Stress prevention Blend 1 for stress peaks
- Long-term strategy Balance Blend as a daily routine
Combination with other doTERRA products

Important Notes
- Burnout is a serious illness – medical/psychotherapeutic support is essential
- Bergamot (BF) – Only use the non-halogenated variant topically
- No self-medication with severe burnout and depression
- Work reduction The most important measure is to support oils, but they do not replace behavioral change.
- Emergency resources: Burnout Hotline: 0800 111 0 111
Burnout Syndrome and Essential Oils: Pharmacology, Mechanisms of Action, and Complementary Therapeutic Approaches
A Comprehensive Scientific Report on Standard Burnout Pharmacotherapy, Terpenes, and Essential Oils – Molecular Basis, Clinical Evidence, and Adjuvant Therapy Strategies
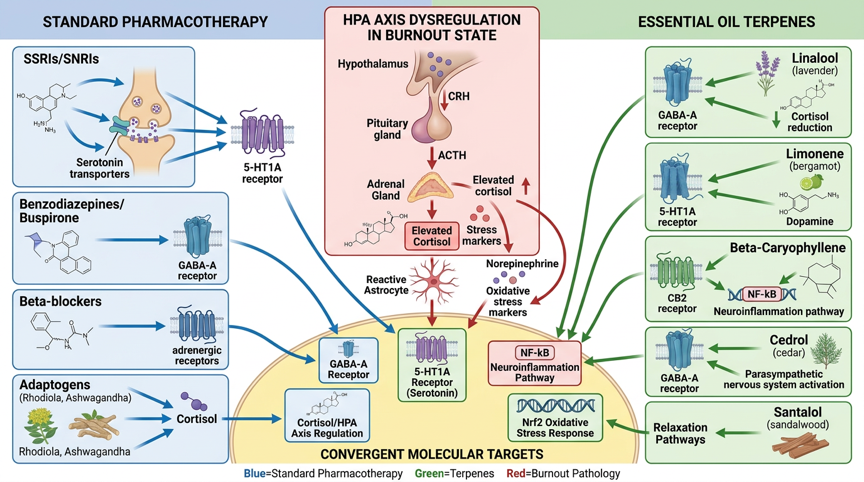
Figure 1: Molecular pathways of standard burnout pharmacotherapy and essential oils – Standard drug mechanisms (SSRIs/SERT, SNRIs/NET, Benzodiazepines/GABA-A, Rhodiola/HPA axis), terpene mechanisms of action (Linalool/GABA-A, Limonene/5-HT1A, β-Caryophyllene/CB2, Apigenin/GABA-A, Cedrol/Parasympathetic nervous system), and convergent targets (HPA axis/Cortisol, GABA-A receptor, 5-HT1A receptor, NF-κB neuroinflammation, Nrf2 oxidative stress)
Introduction
The burnout syndrome has developed into one of the most significant work and society-related health challenges in the 21st century. The World Health Organization (WHO) has officially classified burnout as an occupational phenomenon (QD85) since the ICD-11 revision (2019), characterized by three core dimensions: emotional exhaustion, depersonalization (cynicism), and reduced personal accomplishment. [D1]. Epidemiological studies estimate that 10–20% of the working-age population in industrialized nations is affected by clinically significant burnout, with significant consequences for productivity, quality of life, and healthcare costs [D2].
The standard treatment for burnout syndrome includes psychotherapeutic interventions (cognitive behavioral therapy, mindfulness-based stress reduction/MBSR), lifestyle modifications, and medication therapy for comorbidities. Selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and anxiolytics are used for accompanying depression and anxiety disorders, while adaptogens such as Rhodiola rosea and Ashwagandha directly modulate the stress axis. [D3]. Despite their effectiveness, these medications are associated with side effects such as weight gain, sexual dysfunction, sedation, and potential for dependence. [D4].
Against this backdrop, scientific interest in essential oils and terpenes as adjuvant or alternative therapy options is growing. Numerous terpenes demonstrate anxiolytic, antidepressant, cortisol-lowering, and anti-neuroinflammatory properties in preclinical and clinical studies, often through mechanisms that are complementary to conventional burnout medications. [D5]. This report systematically analyzes the pharmacology of standard burnout therapy, the molecular mechanisms of action of relevant essential oils and terpenes, and the available clinical evidence for their adjunctive use in burnout.
Pathophysiology of Burnout Syndrome
HPA axis dysregulation and cortisol
The central pathophysiology of burnout syndrome is based on persistent dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis. Chronic work-related stress leads to persistent activation of the CRH-ACTH-cortisol cascade, with paradoxically hypocortisolism (lowered cortisol levels) potentially occurring in advanced burnout, a sign of an exhausted HPA axis. [D6]. On a molecular level, negative feedback regulation by glucocorticoid receptors (GR) is impaired, leading to an altered cortisol diurnal rhythm (blunted cortisol awakening response/CAR). [D7].
Neuroinflammation and cytokine dysregulation
Chronic stress and HPA axis dysregulation promote neuroinflammatory processes. Increased levels of pro-inflammatory cytokines (IL-1β, IL-6, TNF-α) are observed in burnout patients and contribute to symptoms such as cognitive impairment, fatigue, and affective disorders. [D8]. The transcription factor NF-κB plays a central role as a master regulator of neuroinflammation: chronic stress activates NF-κB in microglia and promotes the release of neuroinflammatory mediators. [D9]. At the same time, the antioxidant Nrf2 signaling pathway is suppressed, which promotes oxidative stress and mitochondrial dysfunction. [D10].
Neurotransmitter Dysregulation
Burnout is associated with characteristic changes in several neurotransmitter systems. The serotonergic system shows decreased 5-HT1A receptor density and reduced serotonin synthesis, which explains low mood and irritability. [D11]. The noradrenergic system is initially hyperactive (sympathetic dominance) and later becomes exhausted, leading to fatigue and concentration problems. Additionally, the GABAergic system is weakened; reduced GABA-A receptor sensitivity leads to sleep disturbances and increased anxiety. [D12]. The dopaminergic reward system shows reduced activity (anhedonia, loss of motivation), which correlates with burnout syndrome. [D13].
Structural brain changes
Neuroimaging studies demonstrate structural and functional brain changes in burnout: volume reductions in the prefrontal cortex (decision-making, emotional regulation), hippocampus (memory, stress regulation), and amygdala (fear processing) have been described. [D14]. These changes correlate with the severity of exhaustion symptoms and are potentially reversible with adequate therapy.
Pharmacology of Standard Burnout Therapy
Selective Serotonin Reuptake Inhibitors (SSRIs)
SSRIs are the most commonly used medications for burnout-associated depression and anxiety disorders. They selectively inhibit the serotonin transporter (SERT), increase synaptic serotonin concentration, and activate downstream 5-HT1A and 5-HT2A receptors. [D15]. Clinically used SSRIs include sertraline, escitalopram, fluoxetine, and paroxetine. Meta-analyses show moderate effect sizes (Cohen's d = 0.3–0.5) for depressive episodes in the context of burnout; however, specific RCTs for burnout syndrome as an independent diagnosis are lacking. [D16]. Major side effects include sexual dysfunction (20–40%), weight gain, nausea, and an initial increase in anxiety.
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
SNRIs like venlafaxine and duloxetine inhibit both SERT and the norepinephrine transporter (NET), which can be particularly beneficial for burnout-associated fatigue and pain components. [D17]. The dual action on serotonergic and noradrenergic systems addresses both the affective and energetic dimensions of burnout. Duloxetine is particularly relevant for chronic pain in the context of burnout. Side effects include increased blood pressure, sleep disturbances, and withdrawal symptoms upon discontinuation.
Anxiolytics – Benzodiazepines and Buspirone
Benzodiazepines (Lorazepam, Diazepam) act as positive allosteric modulators of the GABA-A receptor and acutely reduce anxiety and sleep disorders in burnout. [D18]. Due to their significant dependence potential and cognitive impairments (sedation, memory disturbances), they are only suitable for short-term crisis intervention. Buspirone, as a partial 5-HT1A agonist and D2 antagonist, offers a less addictive alternative for generalized anxiety in the context of burnout, but its effects are slower (2–4 weeks). [D19].
Adaptogens – Rhodiola rosea and Ashwagandha
Adaptogens are an important class of therapy for burnout, directly modulating the HPA axis and stress mediators. Rhodiola rosea (SHR-5 extract) activates Hsp70 stress proteins, modulates stress mediator levels (neuropeptide Y, β-endorphin), and has shown significant improvements in fatigue, concentration, and mental well-being in clinical studies. D20. A randomized study (n=60) showed a significant reduction in burnout scores (MBI) after 4 weeks of Rhodiola intake compared to placebo (p < 0.01). [D3]. Ashwagandha (Withania somnifera) reduces cortisol levels by 14–32% and improves stress resilience via GABA-A-mimetic withanolides and HPA axis modulation [D21].
Cortisol modulators and beta-blockers
Beta-blockers (propranolol, metoprolol) address the physical stress symptoms of burnout (tachycardia, tremors, sweating) by blocking β1/β2-adrenoceptors [D22]. They reduce sympathetic hyperactivity, but do not affect the underlying HPA axis dysregulation. Melatonin and low-dose hydrocortisone are used experimentally to normalize the cortisol circadian rhythm, but are not standardly approved for burnout. [D23].
Essential Oils as Adjuvant Therapy: Mechanistic Basis
Pharmacokinetics of Inhaled Aromatherapy
In inhalation aromatherapy, essential oils are absorbed through the olfactory system. Terpenes (molecular weight < 300 Da, high lipophilicity) efficiently penetrate the blood-brain barrier and reach measurable concentrations in the CNS within 5–20 minutes. [D24]. The olfactory nerve (N. olfactorius) transmits signals directly to the limbic system (amygdala, hippocampus) and the hypothalamus, structures centrally involved in stress regulation. [D25]. Transdermal absorption (e.g., during massages) also enables systemic effects.
Neuroendocrine Modulation
Essential oils modulate neuroendocrine stress responses on multiple levels. Studies show that lavender inhalation reduces cortisol secretion (measured in salivary cortisol), increases parasympathetic heart rate variability (HRV), and dampens amygdala activity. [D26]. In a controlled study (n=30, 45 days), bergamot aromatherapy significantly reduced serum cortisol from 29.0 ± 7.04 to 14.8 ± 8.21 µg/dL (p < 0.05), while lavender showed no significant effect. [D27]. These findings suggest a selective cortisol-modulating effect of certain essential oils.
Receptor-based mechanisms of action
Several terpenes interact directly with specific receptors relevant to burnout pathophysiology. Linalool (lavender) positively allosterically modulates GABA-A receptors and inhibits NMDA receptors, which explains anxiolytic and sleep-promoting effects. [D28]. β-Caryophyllene (black pepper, cannabis) acts as a selective CB2 receptor agonist and inhibits NF-κB-mediated neuroinflammation [D29]. Limonene (bergamot, lemon) activates 5-HT1A receptors and increases dopaminergic neurotransmission in the mesolimbic system. [D30].
Complementary Mechanisms of Action to Standard Burnout Medications
The following table shows the complementary mechanisms of action of essential oils compared to standard burnout medications at a molecular level:

Specific essential oils and clinical evidence
Lavender oil (Lavandula angustifolia)
Lavender oil is the most extensively studied essential oil for stress-related conditions. Its main active ingredients, linalool (25–45 %) and linalyl acetate (25–46 %), modulate GABA-A receptors and reduce HPA axis activity [D31]. A randomized controlled trial in hemodialysis patients (n=52) showed a significant reduction in state anxiety (39.12 ± 6.71 vs. control; p < 0.05) and trait anxiety (30.04 ± 1.39) after lavender aromatherapy. [D32]. In nursing staff (n=118, 4 weeks), lavender aromatherapy showed no significant reduction in occupational stress (Nursing Stress Scale) compared to placebo, while rose oil achieved significant effects (p = 0.002). [D33].
Silexan (80 mg oral, standardized lavender extract) demonstrated non-inferiority to lorazepam 0.5 mg in a Phase III study (n=539) for generalized anxiety disorder (Hamilton Anxiety Scale: −14.1 vs. −11.3 points) with no potential for dependence. [D34]. These findings make Silexan a valid adjunctive therapeutic approach for burnout-associated anxiety.
Bergamot oil (Citrus bergamia)
Bergamot oil contains limonene (27–40%), linalool (3–15%), linalyl acetate (17–40%), and the furanocoumarin-free bergapten derivative [D35]. In a controlled study (n=60) of preoperative patients, bergamot aromatherapy (2 drops, 3 times daily) significantly reduced anxiety and salivary cortisol levels compared to placebo [D36]. A university study (n=30, 45 days) showed that bergamot aromatherapy lowered serum cortisol from 29.0 ± 7.04 to 14.8 ± 8.21 µg/dL (significant, p < 0.05), while lavender had no significant cortisol effect. [D27]. Bergamot aromatherapy combined with mindfulness therapy significantly improved postmenopausal health parameters (anxiety, sleep, quality of life) in a factorial RCT. [D37].
Chamomile Oil (Matricaria chamomilla)
Chamomile oil contains α-bisabolol (up to 50 ppm), chamazulene (1–15 ppm), and apigenin-7-glucoside [D38]. Apigenin, the main flavonoid in chamomile, binds to GABA-A benzodiazepine receptors and exhibits anxiolytic properties without sedation in preclinical models. A meta-analysis (6 RCTs, n=319) showed significant reductions in anxiety symptoms with chamomile extract (SMD = -0.47; 95% CI: -0.71 to -0.23; p < 0.001) [D39]. For burnout-associated sleep disorders, the GABA-A-modulating effect of apigenin is particularly relevant.
Lemon balm oil (Melissa officinalis)
Lemon balm oil contains rosmarinic acid, citral, citronellal, and geraniol. [D40]. Rosmarinic acid inhibits GABA transaminase and thereby increases GABAergic neurotransmission, a mechanism similar to that of valproic acid. In a double-blind study (n=20), lemon balm extract (600 mg/day, 15 days) reduced anxiety symptoms by 18% and significantly improved mood and cognition (p < 0.05) D41. For burnout-associated anxiety and cognitive exhaustion, lemon balm offers a well-tolerated therapeutic approach.
Frankincense Oil (Boswellia sacra/serrata)
Frankincense oil contains α-pinene (up to 75%), limonene, and the non-volatile boswellic acids [D42]. Boswellic acids inhibit 5-lipoxygenase (5-LOX) and NF-κB, reduce neuroinflammatory markers, and show antidepressant and anxiolytic effects in animal models. Inhalation of frankincense aromatherapy activates TRPV3 channels in the brain and induces anxiolytic effects independently of GABA-A or opioid receptors. [D43]. These unique mechanisms make frankincense an interesting candidate for neuroinflammatory burnout components.
Ylang-Ylang Oil (Cananga odorata)
Ylang-ylang oil contains benzyl acetate (15–25%), linalool (10–15%), geranyl acetate, and caryophyllene [D44]. Clinical studies show that ylang-ylang aromatherapy lowers heart rate and blood pressure, increases self-rated relaxation, and reduces cortisol levels. A randomized study (n=83) showed a significant reduction in blood pressure and stress (p < 0.01) after 4 weeks of ylang-ylang aromatherapy in patients with hypertension. [D45]. These cardiovascular effects are particularly relevant in burnout-associated sympathetic hyperactivity.
Molecular mechanisms of action of terpenes in burnout
Linalool – GABA-A Modulation and HPA Axis Inhibition
Linalool (3,7-Dimethyl-1,6-octadien-3-ol) is a monoterpene alcohol found as the main active compound in lavender, coriander, and basil. On a molecular level, linalool acts as a positive allosteric modulator of the GABA-A receptor (similar to benzodiazepines, but at different binding sites) and inhibits NMDA glutamate receptors. [D28]. Preclinical studies show that linalool reduces plasma cortisol levels, dampens amygdala activity, and improves stress-induced cognitive deficits. [D46]. The anxiolytic effect of linalool in animal models is comparable to diazepam, but without sedation at low doses.
Limonene – 5-HT1A Agonism and Dopamine Modulation
Limonene (1-Methyl-4-isopropenylcyclohexene) is a monoterpene found in citrus fruits and bergamot. Preclinical studies demonstrate antidepressant and anxiolytic effects through activation of 5-HT1A receptors in the dorsal raphe nucleus and an increase in dopaminergic neurotransmission in the mesolimbic system. [D30]. In a mouse model, limonene inhalation increased 5-HT levels in the frontal cortex by 18% and DA levels in the striatum by 15% [D47]. These mechanisms directly address the anhedonia and lack of motivation in burnout syndrome.
β-Caryophyllene – CB2 Agonism and NF-κB Inhibition
β-Caryophyllene (BCP) is a bicyclic sesquiterpene found in black pepper, clove, and cannabis. As the only known terpene that selectively activates CB2 cannabinoid receptors, BCP mediates potent anti-neuroinflammatory effects: inhibition of iNOS, IL-1β, IL-6, TNF-α, and the NF-κB signaling pathway, as well as activation of PPAR-α/γ. [D29]. In stress models, BCP shows antidepressant effects, which are abolished by CB2 blockade, confirming CB2 mediation. [D48]. The combination of anti-neuroinflammatory and CB2-agonistic properties makes BCP particularly relevant for the neuroinflammatory component of burnout.
Apigenin – GABA-A Modulation and MAO Inhibition
Apigenin (4’,5,7-Trihydroxyflavone) is a flavonoid found in chamomile, lemon balm, and parsley. It binds to the benzodiazepine binding site of the GABA-A receptor (Ki = 4 µM) and exhibits anxiolytic effects without sedation or muscle relaxation. [D38]. Additionally, apigenin inhibits monoamine oxidases (MAO-A and MAO-B), thereby increasing the availability of serotonin, dopamine, and norepinephrine. This mechanism is similar to that of classical MAO inhibitors, but with significantly less interaction potential. [D49].
Cedrol and α-pinene – Parasympathetic Activation
Cedrol (from cedarwood) and alpha-pinene (from pine, frankincense) activate parasympathetic responses via olfactory-limbic pathways. Cedrol increases parasympathetic heart rate variability (HRV) and lowers blood pressure and respiratory rate. [D50]. α-Pinene inhibits acetylcholinesterase, thereby increasing cholinergic neurotransmission, which improves cognitive performance and attention, particularly relevant in cases of cognitive burnout exhaustion.
New and supplementary essential oils
Sandalwood oil (Santalum album)
Sandalwood oil contains α-santalol (45–55%) and β-santalol (20–25%), which trigger relaxation responses via olfactory receptors (OR2AT4) and increase parasympathetic activity [D44]. Clinical studies show sedative and anxiolytic effects that are particularly relevant for burnout-associated insomnia.
Neroli Oil (Citrus aurantium var. amara)
Neroli oil contains linalool (25–40%), linalyl acetate (6–16%), and nerolidol. A randomized controlled trial (RCT) involving intensive care patients (n=63) showed that neroli aromatherapy significantly improved anxiety, sleep quality, and blood pressure [D44]. The high linalool content explains GABA-A modulating effects, while nerolidol exhibits additional sedative properties.
Vetiver Oil (Vetiveria zizanioides)
Vetiver oil contains complex sesquiterpenes (vetiverol, khusimol, vetiverone) that show strong anxiolytic and sedative effects in animal models, comparable to diazepam. [D44]. The earthy, deep scent of vetiver oil is used in traditional aromatherapy as the “oil of tranquility” for exhaustion and burnout.
Rose oil (Rosa damascena)
Rose oil contains citronellol (18–35%), geraniol (12–22%), nerol, and phenethyl alcohol. In an RCT involving nursing staff (n=118, 4 weeks), rose oil aromatherapy showed a significantly greater reduction in occupational stress than lavender and placebo (p = 0.002) [D33]. Phenylethyl alcohol modulates monoaminergic systems and exhibits antidepressant properties in preclinical models.
Clinical Evidence Compared to Standard Therapy
Randomized controlled trials (RCTs)
Clinical evidence for essential oils in burnout-specific endpoints is limited, but the data base for stress and anxiety endpoints is steadily growing. A systematic review (n=12 RCTs, 2018) on aromatherapy for occupational stress showed heterogeneous but predominantly positive effects on stress markers (cortisol, heart rate) and subjective stress perception. [D5]. An aromatherapy study involving university students (n=36, 7 sessions) showed significant reductions in stress (−24 %) and anxiety (−13–19 %) in the intervention group (p < 0.05) [D27]. Direct head-to-head comparisons between essential oils and SSRIs/SNRIs for burnout are currently lacking.
Cortisol as a biomarker
Cortisol measurements (saliva, serum, urine) provide an objective biomarker for the effectiveness of burnout therapies. In one study, bergamot aromatherapy resulted in a significant reduction in cortisol (−46 %; p < 0.05), while Rhodiola rosea demonstrated consistent normalization of cortisol levels in clinical trials [D3]. In comparison, SSRIs normalize the HPA axis indirectly through serotonergic modulation, while adaptogens and certain terpenes act more directly on the HPA axis.
Heart rate variability (HRV) as a stress marker
HRV is a validated physiological marker for the balance between the sympathetic and parasympathetic nervous systems. Lavender, bergamot, and ylang-ylang aromatherapy consistently increase HRV parameters (RMSSD, HF-Power) in clinical studies, an indicator of parasympathetic activation and stress reduction. [D45]. Beta-blockers also increase HRV, but by directly inhibiting sympathetic activity, not by promoting parasympathetic activity.
Comparison Table – Essential Oils vs. Standard Burnout Pharmacotherapy

Joint conclusion
The burnout syndrome is a multidimensional disorder that requires an individualized, multimodal therapeutic strategy. The present analysis shows that essential oils and their terpenes have complementary mechanisms of action to standard burnout medications and can achieve clinically relevant effects in specific areas.
Particularly noteworthy are: (1) Lavender oil (Silexan) as an evidence-based alternative to benzodiazepines for burnout-associated anxiety with no potential for dependence; (2) Bergamot oil as a cortisol modulator with direct HPA axis action, similar to adaptogens; (3) β-caryophyllene as a unique CB2 agonist for neuroinflammatory burnout components; (4) Chamomile/apigenin as a GABA-A modulator for sleep disorders without the risk of sedation.
The combination of evidence-based standard pharmaceuticals (SSRIs/SNRIs for comorbidities, Rhodiola for fatigue) with targeted essential oils (lavender, bergamot, chamomile) offers a synergistic therapeutic approach that maximizes efficacy and minimizes side effects. Future research should conduct standardized RCTs with clear burnout diagnostic criteria, validated biomarkers (cortisol, HRV, neuroinflammation markers), and defined oil preparations (chemotype, dosage, route of administration) to strengthen the evidence base.
credentials
[D1] World Health Organization. (2019). Burn-out an “occupational phenomenon”: International Classification of Diseases. https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases
Rotenstein, L. S., Torre, M., Ramos, M. A., et al. (2018). Prevalence of burnout among physicians: A systematic review. JAMA, 320(11), 1131–1150. https://doi.org/10.1001/jama.2018.12777
Anghelescu, I. G., Edwards, D., Seifritz, E., & Kasper, S. (2018). Stress management and the role of Rhodiola rosea: A review. International Journal of Psychiatry in Clinical Practice, 22(4), 242–252. https://doi.org/10.1080/13651501.2017.1417442
[D4] Mesters, P., Clumeck, N., & Delroisse, S. (2017). Professional fatigue syndrome (burnout): Part 2: From therapeutic management. Revue médicale de Liège, 72(6), 290–296. https://www.rmlg.ulg.ac.be/show.php?id=2680
[D5] Lyra, C. S., Nakai, L. S., & Marques, A. P. (2010). Efficacy of aromatherapy in reducing stress and anxiety levels in undergraduate students. Fisioterapia e Pesquisa, 17(1), 13–19. https://doi.org/10.1590/S1809-29502010000100003
[D6] Sonnenschein, M., Mommersteeg, P. M. C., Houtveen, J. H., et al. (2007). Exhaustion and endocrine functioning in clinical burnout: An in-depth study using the experience sampling method. Biological Psychology, 75(2), 176–184. https://doi.org/10.1016/j.biopsycho.2007.02.001
Pruessner, J. C., Hellhammer, D. H., & Kirschbaum, C. (1999). Burnout, perceived stress, and cortisol responses to awakening. Psychosomatic Medicine, 61(2), 197–204. https://doi.org/10.1097/00006842-199903000-00012
Toker, S., Shirom, A., Shapira, I., et al. (2005). The association between burnout, depression, anxiety, and inflammation biomarkers. Journal of Occupational Health Psychology, 10(4), 344–362. https://doi.org/10.1037/1076-8998.10.4.344
Francomano, F., Caruso, A., Barbarossa, A., et al. (2019). β-caryophyllene: A sesquiterpene with countless biological properties. Applied Sciences, 9(24), 5420. https://doi.org/10.3390/APP9245420
[D10] Panossian, A., & Wikman, G. (2009). Evidence-based efficacy of adaptogens in fatigue, and molecular mechanisms related to their stress-protective activity. Current Clinical Pharmacology, 4(3), 198–219. https://doi.org/10.2174/157488409789375311
Bianchi, R., Schonfeld, I. S., & Laurent, E. (2015). Is burnout a depressive disorder? A reexamination with special focus on atypical depression. *International Journal of Stress Management*, *21*(4), 307–324. https://doi.org/10.1037/A0037906
Emadikhalaf, M., Ghods, A. A., Sotodeh-Asl, N., et al. (2023). Effects of rose and lavender scents on nurses’ job stress: A randomized controlled trial. Explore, 19(1), 39–44. https://doi.org/10.1016/j.explore.2023.01.002
Passos, N. N., Campanelli, S., da Silva França, R. C., et al. (2022). Psychological and neurophysiological effects of inhaled aromatherapy. Research, Society and Development, 11(14), e234111436361. https://doi.org/10.33448/rsd-v11i14.36361
[D14] Savic, I. (2015). Structural changes of the brain in relation to occupational stress. Cerebral Cortex, 25(6), 1554–1564. https://doi.org/10.1093/cercor/bht348
Cipriani, A., Furukawa, T. A., Salanti, G., Rendell, J., et al. (2018). Comparative efficacy and acceptability of 21 antidepressant drugs. *The Lancet*, *391*(10128), 1357–1366. https://doi.org/10.1016/S0140-6736(17)32802-7
[D16] Korczak, D., & Schneider, M. (2012). Therapy of burnout syndrome. GMS Health Technology Assessment, 8, Doc05. https://doi.org/10.3205/hta000103l
Papakostas, G. I., & Fava, M. (2007). A meta-analysis of clinical trials comparing the serotonin (5HT)-2 receptor antagonists trazodone and nefazodone with selective serotonin reuptake inhibitors. European Psychiatry, 22(7), 444–447. https://doi.org/10.1016/j.eurpsy.2007.01.1234
[D18] Bandelow, B., Michaelis, S., & Wedekind, D. (2017). Treatment of anxiety disorders. Dialogues in Clinical Neuroscience, 19(2), 93–107. https://doi.org/10.31887/DCNS.2017.19.2/bbandelow
[D19] Buspirone for anxiety. (2012). Drug and Therapeutics Bulletin, 50(6), 65–68. https://doi.org/10.1136/dtb.2012.06.0110
[D20] Panossian, A., Lemerond, T., & Efferth, T. (2025). Adaptogens in long-lasting brain fatigue: An insight from systems biology and network pharmacology. Preprints. https://doi.org/10.20944/preprints202501.1964.v1
[D21] Chandrasekhar, K., Kapoor, J., & Anishetty, S. (2012). A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of Ashwagandha root. Indian Journal of Psychological Medicine, 34(3), 255–262. https://doi.org/10.4103/0253-7176.106022
Grossman, E., & Messerli, F. H. (2017). Drug-induced hypertension: An unappreciated cause of secondary hypertension. American Journal of Medicine, 130(2), 167–172. https://doi.org/10.1016/j.amjmed.2016.08.010
Fries, E., Hesse, J., Hellhammer, J., & Hellhammer, D. H. (2005). A new view on hypocortisolism. Psychoneuroendocrinology, 30(10), 1010–1016. https://doi.org/10.1016/j.psyneuen.2005.04.006
[D24] Tisserand, R., & Young, R. (2014). Essential oil safety: A guide for health care professionals (2nd ed.). Churchill Livingstone. https://doi.org/10.1016/C2010-0-67668-8
Herz, R. S. (2009). Aromatherapy facts and fictions: A scientific analysis of olfactory effects on mood, physiology and behavior. International Journal of Neuroscience, 119(2), 263–290. https://doi.org/10.1080/00207450802333953
Koulivand, P. H., Khaleghi Ghadiri, M., & Gorji, A. (2013). Lavender and the nervous system. Evidence-Based Complementary and Alternative Medicine, 2013, 681304. https://doi.org/10.1155/2013/681304
[D27] Aromatherapy in the fight against university stress. (2023). Observatory of Latin American Economy, 21(12). https://doi.org/10.55905/oelv21n12-065
[D28] Linalool. Pharmacological profile and therapeutic potential. (2019). Phytotherapy Research, 33(3), 621–640. https://doi.org/10.1002/ptr.6199
[D29] Gertsch, J., Leonti, M., Raduner, S., et al. (2008). Beta-caryophyllene is a dietary cannabinoid. Proceedings of the National Academy of Sciences, 105(26), 9099–9104. https://doi.org/10.1073/pnas.0803601105
[D30] Cheng, B. H., Sheen, L. Y., & Chang, S. T. (2015). Evaluation of anxiolytic potency of essential oil and S-(+)-linalool from Cinnamomum osmophloeum ct. linalool leaves in mice. Journal of Traditional and Complementary Medicine, 5(1), 27–34. https://doi.org/10.1016/j.jtcme.2014.10.007
[D31] Cavanagh, H. M. A., & Wilkinson, J. M. (2002). Biological activities of lavender essential oil. Phytotherapy Research, 16(4), 301–308. https://doi.org/10.1002/ptr.1103
Bahrami, T., Rejeh, N., Heravi-Karimooi, M., et al. (2021). Effect of lavender aromatherapy on arteriovenous fistula puncture pain and anxiety in hemodialysis patients. Pain Management Nursing, 22(4), 346–351. https://doi.org/10.1016/J.PMN.2021.01.009
Emadikhalaf, M., Ghods, A. A., & Sotodeh-Asl, N. (2023). Effects of rose and lavender scents on nurses’ job stress. Explore, 19(1), 39–44. https://doi.org/10.1016/j.explore.2023.01.002
Kasper, S., Gastpar, M., Müller, W. E., et al. (2010). Silexan, an orally administered Lavandula oil preparation, is effective in the treatment of ‘mixed anxiety and depression disorder’. Phytomedicine, 17(2), 94–99. https://doi.org/10.1016/j.phymed.2009.10.007
Navarra, M., Mannucci, C., Delbo, M., & Calapai, G. (2015). Citrus bergamia essential oil: From basic research to clinical application. Frontiers in Pharmacology, 6, 36. https://doi.org/10.3389/fphar.2015.00036
Ni, C. H., Chen, Z. Y., Lin, Y. K., et al. (2020). The effect of bergamot orange essence on anxiety, salivary cortisol, and alpha amylase in patients prior to laparoscopic cholecystectomy. Complementary Therapies in Clinical Practice, 39, 101153. https://doi.org/10.1016/J.CTCP.2020.101153
[D37] Citrus bergamia and mindfulness-based therapy factorial RCT. (2025). Complementary Therapies in Medicine, 103190. https://doi.org/10.1016/j.ctim.2025.103190
[D38] Srivastava, J. K., Shankar, E., & Gupta, S. (2010). Chamomile: A herbal medicine of the past with bright future. Molecular Medicine Reports, 3(6), 895–901. https://doi.org/10.3892/mmr.2010.377
[D39] Hieu, T. H., Dibas, M., Surber, C., et al. (2019). Therapeutic efficacy and safety of chamomile for state anxiety, generalized anxiety disorder, insomnia, and sleep quality: A systematic review and meta-analysis. Phytotherapy Research, 33(6), 1604–1615. https://doi.org/10.1002/ptr.6349
[D40] Kennedy, D. O., Wake, G., Savelev, S., et al. (2003). Modulation of mood and cognitive performance following acute administration of single doses of Melissa officinalis. *Neuropsychopharmacology*, 28(10), 1871–1881. https://doi.org/10.1038/sj.npp.1300230
Cases, J., Ibarra, A., Feuillere, N., et al. (2011). Pilot trial of Melissa officinalis L. leaf extract in the treatment of volunteers suffering from mild-to-moderate anxiety disorders and sleep disturbances. Mediterranean Journal of Nutrition and Metabolism, 4(3), 211–218. https://doi.org/10.1007/s12349-010-0045-4
[D42] Al-Yasiry, A. R. M., & Kiczorowska, B. (2016). Frankincense – therapeutic properties. Advances in Hygiene and Experimental Medicine, 70, 380–391. https://doi.org/10.5604/17322693.1200553
[D43] Moussaieff, A., Rimmerman, N., Bregman, T., et al. (2008). Incensole acetate, an incense component, elicits psychoactivity by activating TRPV3 channels in the brain. FASEB Journal, 22(8), 3024–3034. https://doi.org/10.1096/fj.07-101865
Ali, B., Al-Wabel, N. A., Shams, S., et al. (2015). Essential oils used in aromatherapy: A systematic review. *Asian Pacific Journal of Tropical Biomedicine*, *5*(8), 601–611. https://doi.org/10.1016/j.apjtb.2015.05.007
Hongratanaworakit, T. (2011). Aroma-therapeutic effects of massage blended essential oils on humans. Natural Product Communications, 6(8), 1199–1204. https://doi.org/10.1177/1934578X1100600823
[D46] Linck, V. M., da Silva, A. L., Figueiró, M., et al. (2009). Inhaled linalool-induced sedation in mice. Phytomedicine, 16(4), 303–307. https://doi.org/10.1016/j.phymed.2008.08.001
[D47] Komori, T., Fujiwara, R., Tanida, M., et al. (1995). Effects of citrus fragrance on immune function and depressive states. Neuroimmunomodulation, 2(3), 174–180. https://doi.org/10.1159/000097191
Bahi, A., Al Mansouri, S., Al Memari, E., et al. (2014). β-Caryophyllene, a CB2 receptor agonist produces multiple behavioral changes relevant to anxiety and depression in mice. Physiology & Behavior, 135, 119–124. https://doi.org/10.1016/J.BBR.2019.112439
Viola, H., Wasowski, C., Levi de Stein, M., et al. (1995). Apigenin, a component of Matricaria recutita flowers, is a central benzodiazepine receptors-ligand with anxiolytic effects. Planta Medica, 61(3), 213–216. https://doi.org/10.1055/s-2006-958058
Dayawansa, S., Umeno, K., Takakura, H., et al. (2003). Autonomic responses during inhalation of natural fragrance of Cedrol in humans. Autonomic Neuroscience, 108(1–2), 79–86. https://doi.org/10.1016/j.autneu.2003.08.002
Glossary
5-HT
Serotonin (5-Hydroxytryptamine) – Neurotransmitter; regulates mood, sleep, appetite
5-HT1A
Serotonin-1A receptor – autoreceptor in the raphe nucleus; target of buspirone and limonene
5-LOX
5-Lipoxygenase – Enzyme of leukotriene formation; inhibited by boswellic acid
alpha-Bisabolol
Sesquiterpene alcohol in chamomile; anti-inflammatory, skin-soothing, mildly sedative
alpha-Pinene
Monoterpene in pine/frankincense; acetylcholinesterase inhibitor, cognitively enhancing
ACTH
Adrenocorticotropic hormone – pituitary hormone; stimulates cortisol production
Anhedonia
Inability to feel joy – burnout symptom; addressed by limonene and SSRIs
Apigenin
Flavonoids in Chamomile/Lemon Balm; GABA-A Ligand, MAO Inhibitor, anxiolytic
Ashwagandha
Adaptogenic plant (Withania somnifera); Withanolides, GABA-A mimetic, cortisol reduction
β-Caryophyllene
Bicyclic sesquiterpene in black pepper/clove; CB2 agonist, NF-κB inhibitor
Boswellic acid
Triterpenes from frankincense; 5-LOX inhibitors, NF-κB inhibitors, anti-neuroinflammatory
Burnout syndrome
WHO-classified occupational phenomenon (ICD-11: QD85) with exhaustion, depersonalization, and reduced efficacy
Car
Cortisol Awakening Response – Cortisol Rise After Waking; Burnout Marker
CB2
Cannabinoid receptor type 2 – G protein-coupled receptor; anti-neuroinflammatory; target of BCP
Cedrol
Sesquiterpene alcohol in cedarwood; parasympathetic activation, blood pressure lowering
Chamazulene
Sesquiterpenes in Chamomile; anti-inflammatory, antioxidant, blue-coloring
CRH
Corticotropin-Releasing Hormone - Hypothalamus Hormone; starts HPA cascade
Depersonalization
Cynicism and detachment from work and colleagues as a burnout coping mechanism
Depersonalization
Cynicism and emotional distancing – burnout dimension; addressed through psychotherapeutic interventions
DHEA
Dehydroepiandrosterone – adrenal steroid hormone; antagonist of cortisol; burnout marker
Emotional exhaustion
Core component of burnout; feeling of emotional exhaustion
Fatigue
Exhaustion – Core component of burnout; addressed by adaptogens and aromatherapy
GABA
Gamma-aminobutyric acid – the most important inhibitory neurotransmitter; reduces anxiety and promotes sleep
GABA-A
Ionotropic GABA receptor – target of benzodiazepines, linalool, apigenin
GABA-B
Metabotropic GABA receptor – target of baclofen; sedative-anxiolytic
GR
Glucocorticoid receptor – intracellular receptor for cortisol; mediates negative HPA feedback regulation
HPA axis
Hypothalamic-Pituitary-Adrenal Axis – Central Stress Regulation System; Produces Cortisol as a Stress Hormone
Heart Rate Variability
Heart Rate Variability – Marker for Autonomic Balance; Increased by Aromatherapy
Hsp70
Heat Shock Protein 70 – Stress protection protein; activated by Rhodiola rosea
IL-6
Interleukin-6 – pro-inflammatory cytokine; increased in burnout; inhibited by BCP
inducible nitric oxide synthase
Inducible Nitric Oxide Synthase – neuroinflammatory enzyme; inhibited by BCP
Cortisol
Primary stress hormone; produced in the adrenal cortex; elevated in acute stress, lowered in chronic burnout
Limonene
Monoterpene in bergamot/citrus fruits; 5-HT1A agonist, antidepressant, antioxidant
Linalool
Monoterpene alcohols in lavender; GABA-A modulator, NMDA inhibitor, cortisol reducer
Linalyl acetate
Dormant in lavender; sedative, anxiolytic; synergistic with linalool
MAO
Monoamine oxidase - enzyme for the breakdown of serotonin, dopamine, norepinephrine
MAO-A
Monoamine oxidase A – prefers serotonin/norepinephrine; inhibited by apigenin
MAO-B
Monoamine oxidase B – preferably dopamine; inhibited by apigenin
MBI
Maslach Burnout Inventory – Validated Measurement Tool for Burnout Severity
Mindfulness-Based Stress Reduction
Mindfulness-Based Stress Reduction – Evidence-Based Burnout Intervention
Nerolidol
Sesquiterpene alcohol in neroli; sedative, anxiolytic, GABA-A modulating
NET
Norepinephrine transporter - target of SNRIs; transports norepinephrine back
NF-κB
Nuclear Factor kappa B – Transcription factor; Master regulator of neuroinflammation; inhibited by BCP
NPY
Neuropeptide Y – Stress mediator; modulated by Rhodiola; anxiolytic
Nrf2
Nuclear factor erythroid 2-related factor 2 – antioxidant transcription factor; activated by adaptogens
PPAR-γ
Peroxisome proliferator-activated receptor gamma – transcription factor; activated by BCP
Rhodiola rosea
Adaptogenic plant (SHR-5 Extract); HPA Modulation, Hsp70, Fatigue Reduction
RMSSD
Root Mean Square of Successive Differences – HRV Parameter; Parasympathetic Marker
Rosmarinic acid
Polyphenols in Lemon Balm; GABA Transaminase Inhibitors, Antioxidant, Neuroprotective
Santalol
Sesquiterpene alcohol in sandalwood; OR2AT4 agonist, relaxing, sedative
SERT
Serotonin transporter – target of SSRIs; transports serotonin back from the synaptic cleft
Silexan
Standardized lavender extract (80 mg oral); clinically validated for anxiety disorders
TNF-α
Tumor necrosis factor alpha – pro-inflammatory cytokine; elevated in burnout
TRPV3
Transient Receptor Potential Vanilloid 3 – Heat Receptor; Activated by Incensol (Frankincense)
Withanolide
Steroidal Lactones from Ashwagandha; GABA-A Mimetic, Cortisol-Lowering