Table of contents
Updated – May 21, 2026
This post provides a detailed explanation of the role of essential oils compared to standard pharmaceuticals in depression, the rationale behind their effects, and the adjuvant benefits they offer.
The first part is a layman-friendly short summary of the scientific report that follows in the second part, for anyone who wants to learn more about natural support for depression.
In the second part, medical professionals, practitioners, and those interested in medical science will find a comprehensive scientific report on standard antidepressants, terpenes, and essential oils, covering molecular foundations, clinical evidence, and adjuvant therapy strategies, supported by mostly peer-reviewed studies.
Audio version – 12:13
What is depression?
Depression is more than just “sadness” or a bad day. It is a real brain disorder in which certain neurotransmitters (chemicals that allow nerve cells to communicate with each other) become out of balance. Imagine the brain as a complex communication network: in depression, some connections are no longer working properly.
What happens in the brain during depression?
- Serotonin, Norepinephrine, and Dopamine, the so-called “happiness hormones” are too low or are not being used correctly
- The body's stress system (the so-called HPA axis) is permanently overactive, as if one were constantly on high alert.
- Specific brain regions responsible for pleasure and motivation (such as the limbic system) work in a dampened state.
- Chronic inflammatory processes in the brain can worsen mood
How common is depression?
Depression affects about 280 million people worldwide, which is 3.8 % of the world's population. In Germany, around 5 million people suffer from depression requiring treatment. It is one of the most common illnesses overall.
Depression is usually treated with psychotherapy and/or medication.
Antidepressants – the standard medications
Doctors often prescribe medications for depression that affect neurotransmitters in the brain. The best known are:
SSRIs (Selective Serotonin Reuptake Inhibitors)
e.g. Fluoxetine (Prozac), Sertraline, Escitalopram
They prevent serotonin from being “cleaned up” too quickly, thus leaving more of it available in the brain. The effect only sets in after 2–4 weeks. Side effects include nausea, sleep disturbances, sexual dysfunction, and weight gain.
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors)
e.g. Venlafaxine, Duloxetine
They act on two neurotransmitters simultaneously, namely serotonin and norepinephrine, and are particularly effective for depression with physical pain.
Important to know: Antidepressants help sufficiently in about 50-60 % of patients. In 30-40 %, they do not work well enough or cause disruptive side effects. This is the reason why many people look for complementary options.
Essential oils - what are they really?
Essential oils are highly concentrated plant extracts. They are obtained from flowers, leaves, bark, or roots of plants through steam distillation or cold pressing. They contain hundreds of different chemical compounds (so-called Terpene and Phenol), which give the plant its scent and properties, and protect it from herbivores, as well as bacterial, viral, or fungal infections. These active ingredients essentially represent the plant's immune system.
Unlike pharmaceuticals effective against certain bacteria, viruses, or fungi, where resistance can develop and pathogens can no longer be effectively combatted, even with broad-spectrum antibiotics, the active compounds in essential oils are composed of so many „antibiotics,“ etc., that resistance is no longer possible.
This also explains why essential oils are effective even against the multi-resistant „hospital germ“ (MRSA).
How do they get into the brain?
When you smell an essential oil, the fragrance molecules travel directly through the nose to the olfactory nerve. This has a direct connection to the limbic system, the emotional center of the brain. This is the fastest way for an active ingredient to affect the brain, faster than any medication that first has to be digested, thereby already losing effectiveness and additionally burdening all organs involved in metabolism.
Some compounds from essential oils can also enter the bloodstream through the skin (topically) or by inhalation (olfactorily), thus acting systemically throughout the body.
Which essential oils can help with depression?
Lavender - the best-researched mood oil
Lavender (Lavandula angustifolia) is the only essential oil that has been compared to a real antidepressant in clinical studies and performed well.
- What's inside? Mainly linalool (approx. 25–45 %) and linalyl acetate (approx. 25–50 %)
- What is it doing? Linalool affects the same receptor (GABA-A) that sedatives (benzodiazepines) target, but more gently and without the risk of addiction.
- Clinical trial: The lavender oil preparation “Silexan” (80 mg daily, in capsule form) was as effective as sertraline (a commonly prescribed antidepressant) in one study, with significantly fewer side effects.
- How to apply? Aroma diffuser, massage, or as a capsule (Silexan is available as a medical device)
Bergamot - the mood booster
Bergamot (Bergamot orangeis the citrus fruit that gives Earl Grey tea its aroma.
- What's inside? Limonene, Linalool, Bergapten
- What is it doing? Increases serotonin and dopamine, reduces cortisol (the stress hormone) by up to 46 % in studies
- Studies: Aromatherapy with bergamot significantly reduced anxiety in patients before surgery and in psychiatric facilities.
- Attention: Bergaptol makes the skin photosensitive, use bergapten-free variants for the skin or avoid sun exposure!
Chamomile - Gentle Soothing
Camomile (Matricaria chamomillais one of the oldest medicinal herbs in the world.
- What's inside? Apigenin (a flavonoid), Bisabolol, Chamazulene
- What is it doing? Apigenin binds to the same sites in the brain as benzodiazepines (sedatives), but much milder
- Clinical trial: In a randomized study, chamomile extract significantly reduced depression symptoms (p < 0.001) and prevented relapse in 57 % of patients.
Lemon Balm – Stress and Sleep
Melissa (Melissa officinalissmells of lemon and has been used for centuries to combat nervousness.
- What's inside? Rosmarinic acid, citral, geraniol
- What is it doing? An enzyme (GABA-transaminase) that breaks down GABA is inhibited, leaving more of the calming neurotransmitter in the brain.
- Study 300-600 mg of lemon balm extract daily significantly improved mood and cognitive function.
Frankincense – against inflammation and anxiety
Incense (Boswellia sacra / serratahas been used in religious rituals for millennia, and science is now explaining why.
- What's inside? Incensol, α-Pinene, Boswellic acids
- What is it doing? Activates a special receptor (TRPV3) in the brain that can alleviate anxiety and depression; inhibits inflammation in the brain
- Special feature: Frankincense is one of the few essential oils with a direct antidepressant effect in animal models.
Rose oil, ylang-ylang, jasmine
These oils are often used in aromatherapy and studies show:
- Rose oil Reduces cortisol, improves sleep, anxiolytic
- Ylang-Ylang: Lowers blood pressure and heart rate, reduces anxiety
- Jasmin: Stimulating and mood-lifting, positively activates the nervous system
What does science say? – Simply summarized

Important notes for use
How to Use Essential Oils Safely:
- Aroma diffuser 3–5 drops in water, diffuse for 30–60 minutes
- Inhalation 2 drops on a handkerchief, inhale deeply
- Massage Always dilute with a carrier oil (e.g., almond oil), never pure on the skin!
Recommended dilution: 2–3 % (approx. 10–15 drops per 50 ml carrier oil) - Bad 5–10 drops dissolved in a tablespoon of cream or honey, then added to bathwater
What to consider:
- Never apply internally without medical advice
- Never stop taking antidepressants on your own., that can be dangerous
- Essential oils are a Supplement, no substitute for professional treatment
- During pregnancy and breastfeeding: Ask your doctor
- Some oils (bergamot, citrus) make the skin sensitive to light, don't go into the sun
- Children under 3 years old: No essential oils without expert advice
- Epileptics: Caution with rosemary, eucalyptus, and high doses of camphor
Frequently Asked Questions
Can I take lavender oil instead of my antidepressant?
No, not without consulting your doctor first. Lavender can be a helpful supplement, but suddenly stopping antidepressants can lead to serious withdrawal symptoms.
How quickly do essential oils work?
Some effects (relaxation, mood improvement) can occur within minutes. Long-term antidepressant effects require regular use over weeks.
Which oil should I try first?
Lavender is the first choice, the best researched, safe, and well-tolerated by most people.
Do I have to buy expensive oils?
Quality is important: look for 100% % pure essential oils, preferably with a batch-specific analysis certificate (GC/MS).
Inexpensive perfume oils or synthetic fragrances have no therapeutic effect and, due to their synthetic ingredients, can be harmful to health and cause headaches, nausea, etc.
Anyone who wants to learn more about the selection and quality of essential oils will find information in the article „Essential Oils - Odyssey of a Search“found.
Another contribution quotes Prof. Dr. Dr. Dr. med. habil. Hanns Hatt from the Ruhr University Bochum, who in his video „Healing with fragrances“explains the effect of essential oils on the human body in an interesting, entertaining, and yet scientific way.
The document provides a summary in three sentences. It offers a concise overview of the main points discussed. This allows for a quick understanding of the content without needing to read the full text.
- Depression is a brain disorder in which neurotransmitters and the stress system become unbalanced.
- Essential oils, especially lavender, bergamot, and chamomile, can directly influence the brain through the sense of smell and have been shown in scientific studies to have mood-lifting, anxiety-reducing, and anti-inflammatory effects.
- You are a valuable addition to standard therapy, but do not replace it.
This text is based on the scientific report “Depression and Essential Oils: Pharmacology, Mechanisms of Action, and Complementary Therapeutic Approaches” and is for general informational purposes only.
If you experience side effects, consult a doctor or pharmacist.
Pharmacology, mechanisms of action, and complementary therapeutic approaches
A Comprehensive Scientific Report on Standard Antidepressants, Terpenes and Essential Oils, Molecular Basis, Clinical Evidence, and Adjuvant Therapy Strategies
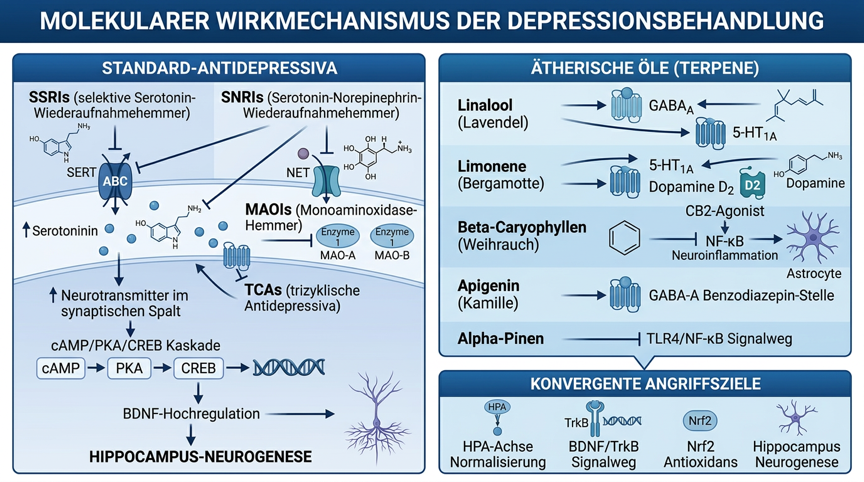
Figure 1: Molecular signaling pathways of antidepressants and essential oils in depression, standard antidepressant mechanisms (SSRIs, SNRIs, TCAs, MAOIs), terpene mechanisms of action (linalool, limonene, β-caryophyllene, apigenin, α-pinene) and convergent targets (HPA axis, BDNF/TrkB, Nrf2, hippocampal neurogenesis)
Introduction
Depression (Major Depressive Disorder, MDD) is one of the most common and disabling psychiatric disorders worldwide. According to the World Health Organization (WHO), over 280 million people suffer from depression, making it a leading cause of disability and lost years of life. [D1]. The illness is characterized by persistent depressive mood, anhedonia, cognitive impairments, sleep disturbances, lack of drive, and in severe cases, suicidality. [D2].
The standard treatment for depression includes psychotherapy (especially cognitive behavioral therapy) and pharmacotherapy with antidepressants. Commonly prescribed drug classes include selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs). [D3]. Trotz ihrer Wirksamkeit sprechen 30–40 % der Patienten nicht auf die erste Behandlungslinie an, und Nebenwirkungen wie sexuelle Dysfunktion, Gewichtszunahme, Schlafstörungen und emotionale Abstumpfung beeinträchtigen die Therapieadhärenz erheblich [D4].
Against this backdrop, scientific and clinical interest in complementary and herbal approaches is growing. Essential oils and their bioactive terpenes show antidepressant, anxiolytic, neuroprotective, and anti-neuroinflammatory properties in preclinical and clinical studies, often through mechanisms of action that are complementary to those of classic antidepressants. [D5]. This report systematically analyzes the pharmacology of standard antidepressants, the molecular mechanisms of action of relevant essential oils and terpenes, and the available clinical evidence for their adjunctive use in depression.
Neurobiology of Depression
Monoamine Hypothesis and its Limitations
The classic monoamine hypothesis of depression postulates that a functional insufficiency of serotonin (5-HT), norepinephrine (NA), and dopamine (DA) in central synaptic clefts causes the core symptoms of depression. [D3]. This hypothesis forms the rational basis for most pharmacological interventions. However, it does not fully explain the delayed response to antidepressants (2–4 weeks), even though transporter blockade begins within hours, suggesting downstream neuroplastic adaptation processes as the actual basis of action. [D6].
Neuroinflammation and the HPA axis
Recent research emphasizes the role of neuroinflammation and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis in the pathophysiology of depression. Elevated levels of pro-inflammatory cytokines (IL-6, TNF-α, IL-1β) and hyperactivity of the HPA axis with consequently increased cortisol levels are well-documented in patients with depression. [D7]. These findings open new therapeutic targets that go beyond classical monoamine systems and explain why substances with anti-neuroinflammatory properties, such as certain terpenes, can be clinically relevant.
BDNF and Neuroplasticity
The neurotrophic factor BDNF (Brain-Derived Neurotrophic Factor) plays a central role in the neuroplasticity hypothesis of depression. Reduced BDNF levels in the hippocampus and prefrontal cortex have been consistently demonstrated in depressed patients; all effective classes of antidepressants increase BDNF expression through various signaling pathways. [D8]. The promotion of hippocampal neurogenesis and synaptic plasticity is considered a common endpoint of many antidepressant interventions today.
Glutamatergic and GABAergic Systems
The Excitatory/Inhibitory (E/I) balance between glutamate and GABA is disturbed in depression. Ketamine, an NMDA receptor antagonist, shows rapid antidepressant effects and has increased interest in glutamatergic mechanisms. [D9]. GABAergic deficits, particularly reduced parvalbumin-positive interneuron activity, contribute to cognitive symptoms. These findings are particularly relevant for essential oils, whose main components (e.g., linalool, apigenin) directly modulate GABAergic systems.
Pharmacology of Standard Antidepressants
Selective Serotonin Reuptake Inhibitors (SSRIs)
SSRIs are the most commonly prescribed antidepressants worldwide. Their primary action is the highly selective blockade of the serotonin transporter (SERT), which leads to increased synaptic 5-HT levels. [D10].
Important SSRIs and their properties:

Transporter Occupancy and Brain Concentrations
Crucial for in vivo efficacy is not the total brain concentration, but the free (unbound) brain concentration, which correlates with SERT occupancy [D11]. Studies show that SERT occupancy at therapeutic doses is ~80 %, a threshold that appears to be necessary for clinical efficacy [D12]. Active metabolites, such as norfluoxetine (after fluoxetine), can prolong SERT inhibition and increase extracellular 5-HT in the frontal cortex. [D13].
Downstream signaling pathways
Chronic SERT blockade → ↑ synaptic 5-HT → Desensitization of presynaptic 5-HT1A autoreceptors → enhanced postsynaptic serotonin signaling → Activation of cAMP/PKA/CREB cascade → ↑ BDNF expression → Hippocampal neurogenesis [D8].
Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
SNRIs inhibit both SERT and the norepinephrine transporter (NET), thus offering a broader spectrum of action that is particularly advantageous for depression with somatic pain symptoms. [D14].

Tricyclic Antidepressants (TCAs)
TCAs are among the oldest antidepressants and exhibit a broad receptor profile: inhibition of SERT and NET plus antagonistic effects at histamine H1, muscarinic, and α1-adrenergic receptors [D16]. This profile explains both the antidepressant efficacy and the significant side effects (sedation, anticholinergic effects, cardiotoxic potential).
Important TCAs
Amitriptyline, Clomipramine, Imipramine, Nortriptyline. Clomipramine shows the strongest SERT affinity of all TCAs and is the drug of choice for obsessive-compulsive disorder. [D16].
Monoamine oxidase inhibitors (MAOIs)
MAOIs inhibit the enzymes MAO-A (preferentially 5-HT, NA) and/or MAO-B (preferentially DA, phenylethylamine), leading to increased synaptic monoamine levels. [D17]. Irreversible MAOIs (Phenelzine, Tranylcypromine) require strict dietary restrictions (low-tyramine diet) due to the risk of hypertensive crisis. Reversible, selective MAO-A inhibitors (Moclobemide) are better tolerated.
Newer antidepressants
Mirtazapine
Noradrenergic and specific serotonergic antidepressant (NaSSA); blocks presynaptic α2-autoreceptors and 5-HT2/5-HT3 receptors. Pronounced sedative and appetite-stimulating effect [D18].
Bupropion
Dopamine and norepinephrine reuptake inhibitors (DNRIs); particularly suitable for depression with lack of drive, also approved for smoking cessation [D18].
Agomelatine
Melatonin-MT1/MT2 agonist and 5-HT2C antagonist; normalizes circadian rhythms; favorable side effect profile [D18].
Esketamine (Spravato): NMDA receptor antagonist; approved for treatment-resistant depression; shows rapid antidepressant effects within hours [D9].
Essential Oils as Adjuvant Therapy - Mechanistic Basis
Olfactory and Limbic Processing
Essential oils primarily work through the olfactory pathway: inhaled terpenes bind to olfactory receptors in the olfactory epithelium → olfactory nerves → olfactory bulb → limbic system (amygdala, hippocampus, prefrontal cortex), regions directly involved in emotional regulation, memory, and mood. [D19]. This direct access to the limbic system without passing through the blood-brain barrier allows for rapid central nervous system effects.
Nose-to-Brain Delivery Recent research has shown that monoterpenes can reach the brain directly through nasal application, opening up new formulation strategies for terpenes with antidepressant effects. D20.
Pharmacological targets
Essential oils and their terpenes interact with a broad spectrum of molecular targets relevant to the pathophysiology of depression:

Complementary Mechanisms of Action for Antidepressants
The plausibility of an adjuvant therapy with essential oils is based on complementary, non-redundant mechanisms of action. While classical antidepressants primarily act on monoamine transporters (SERT, NET) or MAO enzymes, essential oils and terpenes address additional pathomechanisms of depression: GABAergic dysfunction, HPA axis hyperactivity, neuroinflammation, and oxidative stress. [D5].
Synergistic approaches:
- SSRI + Linalool (Lavender): SSRIs increase synaptic 5-HT by blocking SERT; linalool additionally activates 5-HT1A receptors and modulates GABA-A – complementary reduction of anxiety symptoms often comorbid with depression [D21]
- SNRI + Beta-Caryophyllene SNRIs normalize monoamine levels; β-caryophyllene, as a CB2 agonist, inhibits NF-κB-mediated neuroinflammation – addressing the inflammatory subtype of depression [D22]
- TCA + Bergamot: TCAs block multiple receptors; limonene from bergamot activates 5-HT1A and modulates dopamine D2 – potential enhancement of antidepressant effects [D23]
Specific essential oils and clinical evidence
Lavender (Lavandula angustifolia)
Lavender is the most researched essential oil in psychiatry. The standardized oral lavender oil preparation Silexan (80 mg/day) was directly compared with sertraline (50 mg/day) and placebo in a multicenter, double-blind RCT [D24]:
- Primary endpoint (MADRS reduction): Silexan -12.1 points vs. Sertraline -12.6 points vs. Placebo -9.95 points
- Response Rate: ~53–54 % (Silexan and Sertraline) vs. 41.5 % (Placebo)
- Remission rate ~44–45 % (active arms) vs. 32.6 % (placebo)
- Conclusion: Silexan showed statistically significant superiority over placebo and no significant difference compared to sertraline on the primary endpoint. [D24]
Main active ingredients
Linalool (25–45 %)
Linalyl acetate (25–46 %)
Terpinen-4-ol, Ocimene
Molecular Mechanisms
– Modulation of monoaminergic and neuroendocrine systems [D25]
GABA-A receptor modulation (anxiolytic) [D21]
– 5-HT1A activation (antidepressant) [D21]
– HPA axis normalization (cortisol reduction) [D25]
– Anti-neuroinflammatory, antioxidant [D25]
– BDNF upregulation in animal models [D25]
Clinical studies
– Silexan vs. Lorazepam (RCT): comparable anxiolytic efficacy, better tolerated [D26]
Lavender as an adjunct to venlafaxine: no significant added benefit over placebo in a study [D27]
– Inhaled oxytocin for postpartum depression: significant EPDS reduction vs. control [D28]
BergamotBergamot orange)
Main active ingredients
Limonene (approx. 30 %)
Linalyl acetate (approx. 30 %)
Linalool (approx. 12 %)
bergapten-containing furanocoumarins
In aromatherapy, bergamot is traditionally used for depression and anxiety. [D29].
Molecular Mechanisms
– Limonene: Activation of 5-HT1A receptors, dopamine D2 modulation, BDNF upregulation, HPA normalization in chronic stress models [D30]
– Linalool: GABAergic and serotonergic modulation (see above)
- Bergapten: MAO inhibition (in vitro) [D29]
– Anti-neuroinflammatory: Reduction of hippocampal IL-6 and TNF-α in animal models [D29]
Clinical evidence
– Inhalation in psychiatric patients: significant reduction in anxiety and positive mood effect [D31]
– Bergamot aromatherapy before surgery: significant anxiolysis vs. control [D31]
CamilleMatricaria chamomilla / Chamaemelum nobile)
Main active ingredients
Apigenin (Flavonoid)
alpha-Bisabolol
Chamazulene
Matricin.
Apigenin is a potent ligand at the GABA-A benzodiazepine binding site. [D32].
Molecular Mechanisms
- Apigenin: GABA-A benzodiazepine site → anxiolytic, sedative (similar to benzodiazepines, but without addiction potential) [D32]
- alpha-Bisabolol: Anti-inflammatory, neuroprotective
- Chamazulene COX inhibition, anti-neuroinflammatory [D32]
– HPA Axis Modulation: Reduction of Cortisol Release in Stress Models
Clinical evidence
– Chamomile extract (220 mg/day, 8 weeks) vs. placebo in GAD: significant reduction in HAM-A score (p<0.001) [D33]
– Long-term RCT (26 weeks): Chamomile extract reduced relapse rate in remitters [D33]
– Antidepressant effect in animal models: comparable to imipramine in the forced swim test [D32]
Lemon balmMelissa officinalis)
Main active ingredients
Citral
Citronellal
Geraniol
Rosemary acid
The plant has a long tradition in the treatment of anxiety and depression. [D34].
Molecular Mechanisms
MAO-A and MAO-B Inhibition (Rosmarinic acid, Ursolic acid) [D34]
– GABA transaminase inhibition → increased GABA levels [D34]
Acetylcholinesterase inhibition (cognitive enhancement) [D34]
– Antioxidant: Nrf2 activation, reduction of oxidative stress [D34]
Clinical evidence
– 8-week RCT: Melissa officinalis vs. Lavandula vs. Fluoxetine (n=45): similar HAM-D reductions in all three arms [D35]
– Lemon balm extract for mild to moderate depression: significant improvement vs. placebo in several studies [D34]
Frankincense (Boswellia sacra / B. serrata)
Main active ingredients
Incensol acetate
alpha-Pinene
Limes
Boswellic acids
Incensol acetate activates TRPV3 channels and shows anxiolytic and antidepressant effects in animal models [D36].
Molecular Mechanisms
- Incensol acetate TRPV3 activation → anxiolytic, antidepressant in mouse models [D36]
- Boswellic acids 5-Lipoxygenase inhibition → anti-neuroinflammatory
- alpha-Pinene: TLR4/MYD88/NF-κB inhibition → anti-neuroinflammatory [D37]
– Serotonergic Modulation: Increase in Hippocampal 5-HT Levels in Animal Models [D36]
Ylang-YlangCananga odorata)
Main active ingredients
Benzyl acetate
Linalool
Geranyl acetate
β-Caryophyllene
It is traditionally used for anxiety, depression, and emotional stress. [D38].
Molecular Mechanisms
– Linalool component: GABA-A and 5-HT1A (see above)
– β-Caryophyllene: CB2 agonism, NF-κB inhibition, sedative-anxiolytic: Reduction of heart rate and blood pressure in human studies [D38]
– Mood-enhancing: significant increase in self-reports of relaxation and well-being [D38]
Bergamot mint and neroliBitter orange)
Neroli oil contains linalool (approx. 34 %), linalyl acetate (approx. 6 %), limonene, nerolidol, and geraniol [D39].
Molecular Mechanisms
– Linalool/Linalyl acetate: GABA-A and 5-HT1A
– Nerolidol: Anxiolytic in animal models, potentiates pentobarbital sedation
Clinical evidence
- Neroli inhalation in intensive care patients: significant reduction in anxiety and blood pressure [D39]
– Neroli for menopausal symptoms: significant improvement in depression and sexual function [D39]
Clary sageClary sage)
Main active ingredients
Linalyl acetate (60–70 %)
Linalool (10–25 %)
Sclareol
alpha-Terpineol [D40].
Molecular Mechanisms
– Linalyl acetate: GABAergic, serotonergic modulation
- Antidepressant effect Inhaling clary sage increased dopamine levels and reduced cortisol in human studies [D40]
- 5α-Reductase inhibition by sclareol: hormonal modulation relevant for postpartum and perimenopausal depression [D40]
Rose oilRosa damascena)
Main active ingredients
Citronellol (18–55 %)
Geraniol (10-22 %), Nerol, Rosoxide, and Phenylethyl Alcohol D41.
Molecular Mechanisms
– Phenylethyl alcohol: MAO inhibition, dopamine release
– Geraniol: 5-HT1A agonism in docking studies D41
Clinical evidence
– Rose oil inhalation for postpartum depression: significant EPDS reduction vs. control D41
– Rose Oil Foot Bath: Reduction of Anxiety and Depression in Postpartum Women D41
Jasmine (Jasminum grandiflorum / officinale)
Jasmine oil contains benzyl acetate (approx. 25 %), linalool, benzyl benzoate, and indole. [D42].
Molecular Mechanisms
– Benzyl acetate: stimulating, mood-lifting
Linalool: GABA-A, 5-HT1A
- Activating effect Jasmine inhalation increased beta wave activity in the EEG (alertness, positive mood), the opposite of the sedative lavender effect [D42]
– Jasmine as an adjuvant: Combined with lavender for balanced anxiolytic-activating effect [D42]
SandalwoodSantalum album / spicatum)
Main active ingredients
α-Santalol (approx. 50 %)
β-Santalol (approx. 20 %)
Sandalwood [D43].
Molecular Mechanisms
- alpha-Santalol: 5-HT1A agonism (docking studies), sedative-anxiolytic
– Santalol: Activation of olfactory receptors → limbic modulation
Clinical Evidence: Sandalwood Inhalation: Reduction of Anxiety and Improvement of Well-being in Human Studies [D43]
Vetiver (Vetiver)
Main active ingredients
Vetiverol
Khusimol, α-Vetivone, and β-Vetivone [D44].
Molecular Mechanisms
– Earthy, deep scent notes: calming, centering
- Anxiolytic Inhalation reduces anxiety scores in animal studies comparable to diazepam [D44]
– GABA-A Modulation by Khusimol [D44]
- ADHD Data: Vetiver showed improvements in attention and concentration in a pilot study, suggesting CNS-activating components. [D44]
CedarwoodAtlas Cedar / Eastern Redcedar)
Main active ingredients
Cedrol
Alpha-Cedrene
Thujopsene
beta-Cedrene [D45].
Molecular Mechanisms
- Cedrol Sedative, anxiolytic; inhalation prolongs sleep time in animal models
GABA-A Modulation by Cedrol [D45]
– Serotonergic activation: Increase in hippocampal 5-HT levels in rats [D45]
Clinical evidence
– Cedrol inhalation: Reduction of heart rate and sympathetic activity → anti-stress effect [D45]
Frankincense / Weihrauch (Boswellia) — Deep Dive
In addition to the above-mentioned mechanisms, frankincense oil shows particular relevance for the inflammatory subtype of depression. [D36]:
- Inhibition of 5-lipoxygenase → Reduction of leukotriene B4 → anti-neuroinflammatory
- Incubation with boswellic acids reduces IL-6 and TNF-α in microglial cells
- Incensole acetate activates PPARγ → Neuroprotection
Molecular Mechanisms of Terpenes in Depression
Linalool
Linalool is the main active ingredient in lavender, coriander, bergamot, and clary sage, and is considered one of the best-researched monoterpenes with antidepressant effects. [D25].
Mechanisms of action
- GABA-A Modulation: Linalool potentiates GABA-A receptor activity via allosteric binding → anxiolytic, sedative [D21]
- 5-HT1A agonism Activation of presynaptic 5-HT1A autoreceptors → antidepressant-anxiolytic [D21]
- HPA axis normalization: Reduction of cortisol levels in chronic stress models [D25]
- BDNF upregulation: Increased hippocampal BDNF expression → Neuroplasticity [D25]
- Monoaminergic Modulation Modulation of Serotonin, Norepinephrine, and Dopamine Systems [D25]
- Anti-neuroinflammatory Reduction of IL-6, TNF-α, and NF-κB activity [D25]
Clinical relevance
Linalool's use as a therapeutic tool in depression treatment is evaluated as promising in a recent review, showing efficacy in multiple preclinical models (Forced Swim Test, Tail Suspension Test, Chronic Unpredictable Stress). [D25].
Limonene
Limonene is the main terpene in citrus oils (bergamot, lemon, orange) and shows robust antidepressant effects in animal models [D30].
Mechanisms of action
- 5-HT1A Activation Direct interaction with 5-HT1A receptors → antidepressant [D30]
- Dopamine D2 Modulation Dopaminergic transmission modulation → Improvement of anhedonia [D30]
- HPA Normalization Inhalation of limonene normalized HPA hyperactivity in chronic stress models [D30]
- BDNF upregulation: Increase in hippocampal BDNF and receptor expression [D30]
- Monoamine Restoration: Normalization of 5-HT, DA, and NA after chronic stress [D30]
β-Caryophyllene
Beta-caryophyllene (BCP) is a sesquiterpene found in frankincense, black pepper, basil, and cannabis. It is the only known terpene that acts as a selective CB2 receptor agonist. [D22].
Mechanisms of action
- CB2 agonism: Activation of the endocannabinoid system → anti-neuroinflammatory, neuroprotective [D22]
- NF-κB inhibition Reduction of pro-inflammatory cytokines (IL-6, TNF-α, IL-1β) [D22]
- GABAergic Modulation Benzodiazepine-insensitive GABA-A interaction → anxiolytic [D22]
- Serotonergic Interaction: Modulation of 5-HT Systems in Animal Models [D22]
- Nitric oxide inhibition Reduction of NO-synthase activity → neuroprotective [D22]
Special relevance
β-Caryophyllene addresses the inflammatory subtype of depression, a clinically significant subgroup (~30% % of depressed patients) with elevated cytokine levels that respond poorly to classic antidepressants [D7].
alpha-Pinene
Alpha-pinene is a monoterpene found in frankincense, eucalyptus, rosemary, and pine needles [D37].
Mechanisms of action
- TLR4/MYD88/NF-κB inhibition: Anti-neuroinflammatory in the hippocampus [D37]
- Anxiolytic Significant reduction of anxiety-like behavior in animal models [D37]
- Acetylcholinesterase Inhibition Cognitive training, relevant for cognitive symptoms of depression [D37]
- Neuroprotective Reduction of hippocampal neurodegeneration in stress models [D37]
Apigenin
Apigenin is a flavonoid from chamomile, parsley, and celery, a highly selective ligand at the GABA-A benzodiazepine binding site. [D32].
Mechanisms of action
- GABA-A Benzodiazepine Site Anxiolytic with no potential for dependence [D32]
- 5-HT1A partial agonism Antidepressant component [D32]
- MAO Inhibition Increase in monoaminergic neurotransmitters [D32]
- Antioxidant/anti-neuroinflammatory: Nrf2 activation [D32]
Geraniol and Citronellol
Geraniol and citronellol are monoterpene alcohols from rose oil, palmarosa, and lemongrass D41.
Mechanisms of action
- 5-HT1A agonism (Docking Studies for Geraniol) D41
- MAO Inhibition In-vitro data for both compounds D41
- Anti-neuroinflammatory Reduction of microglial activation D41
New and supplementary essential oils
Eucalyptus (Eucalyptus globulus / radiata)
Main active ingredients
1,8-Cineole (Eucalyptol, approx. 70–85 %)
Alpha-pinene and limonene.
Molecular Mechanisms
- 1,8-Cineole Acetylcholinesterase inhibition → cognitive enhancement; anti-neuroinflammatory via NF-κB inhibition [D46]
– Anxiolytic in animal models; improvement of cognitive performance in human studies [D46]
Neuroprotective: Reduction of oxidative stress in the hippocampus [D46]
RosemaryRosemary)
Main active ingredients
1,8-Cineole (Chemotyped Cineole)
Camphor
alpha-Pinene
Borneon.
Molecular Mechanisms
- 1,8-Cineole Cognitive activation, AChE inhibition [D47]
– Mood-boosting: Inhalation improved speed and accuracy in cognitive tests [D47]
– Antioxidant, anti-neuroinflammatory [D47]
Peppermint (Mentha × piperita)
Main active ingredients
Menthol (approx. 40 %)
Menthone
1,8-Cineole
Menthyl acetate.
Molecular Mechanisms
- Menthol: TRPM8 activation → refreshing, attention-boosting
- Cognitive Activation: Improving memory and alertness [D48]
– Mood-boosting: Reduction of fatigue and frustration [D48]
GingerGinger)
Ginger oil contains zingiberene, β-sesquiphellandrene, gingerol, and shogaol.
Molecular Mechanisms
- Anti-neuroinflammatory Inhibition of NF-κB and pro-inflammatory cytokines [D49]
- Antioxidant Nrf2 activation, ROS reduction [D49]
- Serotonergic Modulation 5-HT3 antagonism, 5-HT4 agonism [D49]
Clinical evidence
- Ginger extract improved depressive symptoms in animal models; initial human studies show anxiolytic effects [D49]
Clinical Evidence Compared to Standard Therapy
Meta-analytic evidence
A systematic meta-analysis of aromatherapy RCTs in depression showed a moderate pooled effect on depressive symptoms (standardized mean difference SMD = −0.56; 95 % CI: −0.69 to −0.43) compared to control conditions [D50]. Inhalation and blend oils showed greater effects than single oils in subgroup analyses. [D50].
Silexan vs. Sertraline (Flagship Study)
The most important study to date compared standardized oral lavender oil Silexan (80 mg/day) directly with sertraline (50 mg/day) and placebo over 8 weeks in patients with a major depressive episode. [D24]:

Conclusion: Silexan was not statistically worse than Sertraline on the primary endpoint—a remarkable finding that positions lavender oil as a potential alternative for mild to moderate depression [D24].
Chamomile vs. Placebo (Long-term RCT)
In a 26-week RCT, chamomile extract (220 mg/day) significantly reduced not only acute depression and anxiety symptoms but also the relapse rate after remission compared to placebo. [D33].
Melissa + Lavender vs. Fluoxetine
An 8-week double-blind pilot study (n=45) compared Melissa officinalis, Lavandula angustifolia, and Fluoxetine: similar HAM-D reductions in all three arms, with no significant group differences — limited by the absence of a placebo group and small sample size. [D35].
Evidence gaps and limitations
- Missing placebo controls in many studies
- Heterogeneous Formulations Inhalation vs. Oral vs. Topical
- Small sample sizes in most studies
- Short study duration (mostly 4–8 weeks)
- Missing long-term data for safety
- Nur Silexan has Phase III evidence; other oils only have Phase II or pilot studies
Comparison Chart – Essential Oils vs. Standard Antidepressants

Joint conclusion
Depression is a neurobiologically complex illness that benefits from a multimodal treatment approach. The present analysis shows:
Strengths of available evidence:
- Robust mechanistic data
Linalool, Limonene, β-Caryophyllene, Apigenin, and α-Pinene have well-characterized molecular target structures (GABA-A, 5-HT1A, CB2, NF-κB, TLR4) that act complementarily to classical antidepressants. - Phase III evidence for Silexan
Standardized lavender oil Silexan showed comparable efficacy to sertraline in mild to moderate depression in a direct comparison study. - Inexpensive security profile
Essential oils show fewer sexual side effects, less weight gain, and no potential for dependence in clinical studies. - Addressing Neuroinflammation
Beta-caryophyllene and other terpenes target the inflammatory subtype of depression, which responds poorly to classic antidepressants.
Weaknesses and evidence gaps:
- Missing approval studies for most essential oils (except Silexan)
- Heterogeneous Formulations hinder comparability
- Missing long-term data for safety and efficacy
- Standardization problems with natural products
Clinical practice recommendations:
- Silexan (80 mg/day oral)
Can be considered as an alternative to SSRIs for mild to moderate depression (Phase III evidence) - Adjuvant Aromatherapy
Lavender, Bergamot, Chamomile as complementary measures for anxiety-depression comorbidity - Beta-caryophyllene-rich oils:
In inflammatory subtype of depression (elevated CRP, IL-6) - Prefer standardized extracts
Reproducibility and safety with non-standardized oils
The integration of essential oils into a multimodal treatment concept, complementary to psychotherapy and, if necessary, pharmacotherapy. Essential oils offer a promising, patient-centered approach to treating depression.
credentials
[D1] World Health Organization. (2023). Depressive disorder (depression). WHO Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/depression
[D2] American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425596
Frazer A. (2001). Serotonergic and noradrenergic reuptake inhibitors: prediction of clinical effects from in vitro potencies. The Journal of Clinical Psychiatry, 62(Suppl 12), 16–23.
Rush AJ, Trivedi MH, Wisniewski SR, et al. (2006). Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. American Journal of Psychiatry, 163(11), 1905–1917. https://doi.org/10.1176/ajp.2006.163.11.1905
[D5] Fonseca ECM, Ferreira LR, Figueiredo PLB, et al. (2023). Antidepressant Effects of Essential Oils: A Review of the Past Decade (2012–2022) and Molecular Docking Study of Their Major Chemical Components. International Journal of Molecular Sciences, 24(11), 9244. https://doi.org/10.3390/ijms24119244
Nestler EJ, Barrot M, DiLeone RJ, et al. (2002). Neurobiology of depression. Neuron, 34(1), 13–25. https://doi.org/10.1016/S0896-6273(02)00653-0
[D7] Miller AH, Raison CL. (2016). The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nature Reviews Immunology, 16(1), 22–34. https://doi.org/10.1038/nri.2015.5
[D8] Castrén E, Monteggia LM. (2021). Brain-Derived Neurotrophic Factor Signaling in Depression and Antidepressant Action. Biological Psychiatry, 90(2), 128–136. https://doi.org/10.1016/j.biopsych.2021.05.008
Abdallah CG, Sanacora G, Duman RS, Krystal JH. (2018). The glutamate hypothesis of depression: systematic review of glutamate levels and efficacy of treatments targeting the glutamate system. Depression and Anxiety, 35(3), 223–233. https://doi.org/10.1002/da.22717
Stahl SM. (2013). Stahl’s Essential Psychopharmacology: Neuroscientific Basis and Practical Applications (4th ed.). Cambridge University Press. https://doi.org/10.1017/CBO9781139170956
Liu X, Vilenski O, Kwan J, et al. (2009). Unbound brain concentration determines receptor occupancy: a correlation of drug concentration and brain serotonin and dopamine reuptake transporter occupancy for eighteen compounds in rats. Drug Metabolism and Disposition, 37(7), 1548–1556. https://doi.org/10.1124/DMD.109.026674
[D12] Geldof M, Freijer J, van Beijsterveldt L, et al. (2008). Pharmacokinetic–pharmacodynamic modeling of fluvoxamine 5-HT transporter occupancy in rat frontal cortex. British Journal of Pharmacology, 155(2), 178–188. https://doi.org/10.1038/BJP.2008.179
[D13] Qu Y, Aluisio L, Lord B, et al. (2009). Pharmacokinetics and pharmacodynamics of norfluoxetine in rats: Increasing extracellular serotonin level in the frontal cortex. Pharmacology, Biochemistry and Behavior, 92(3), 497–501. https://doi.org/10.1016/J.PBB.2009.01.023
Kessler RC, Berglund P, Demler O, et al. (2003). The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA, 289(23), 3095–3105. https://doi.org/10.1001/jama.289.23.3095
[D15] Millan MJ, Gobert A, Lejeune F, et al. (2001). S33005, a novel ligand at both serotonin and norepinephrine transporters: I. receptor binding, electrophysiological, and neurochemical profile in comparison with venlafaxine, reboxetine, citalopram, and clomipramine. Journal of Pharmacology and Experimental Therapeutics, 298(2), 565–580.
[D16] Gillman PK. (2007). Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. British Journal of Pharmacology, 151(6), 737–748. https://doi.org/10.1038/sj.bjp.0707253
Youdim MBH, Edmondson D, Tipton KF. (2006). The therapeutic potential of monoamine oxidase inhibitors. Nature Reviews Neuroscience, 7(4), 295–309. https://doi.org/10.1038/nrn1883
[D18] Cipriani A, Furukawa TA, Salanti G, et al. (2018). Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet, 391(10128), 1357–1366. https://doi.org/10.1016/S0140-6736(17)32802-7
[D19] Herz RS. (2009). Aromatherapy facts and fictions: a scientific analysis of olfactory effects on mood, physiology and behavior. International Journal of Neuroscience, 119(2), 263–290. https://doi.org/10.1080/00207450802333953
[D20] Ramos GS, Valim ACSM, Brito MVC, et al. (2025). Nose-to-Brain Delivery System for Incorporating Monoterpenes with Anti-Depressant Potential. Current Neuropharmacology. https://doi.org/10.2174/011570159X380176251215113303
[D21] López V, Nielsen B, Solas M, et al. (2017). Exploring Pharmacological Mechanisms of Lavender (Lavandula angustifolia) Essential Oil on Central Nervous System Targets. Frontiers in Pharmacology, 8, 280. https://doi.org/10.3389/FPHAR.2017.00280
Oliveira GLSD, Silva J, da Silva APCSL, et al. (2020). Anticonvulsant, Anxiolytic and Antidepressant Properties of β-caryophyllene in Swiss Mice: Involvement of Benzodiazepine-GABAAergic, Serotonergic and Nitrergic Systems. Current Molecular Pharmacology, 13(4), 285–297. https://doi.org/10.2174/1874467213666200510004622
[D23] Zhang N, Yao L. (2019). Anxiolytic Effect of Essential Oils and Their Constituents: A Review. Journal of Agricultural and Food Chemistry, 67(50), 13790–13808. https://doi.org/10.1021/ACS.JAFC.9B00433
Kasper S, Anghelescu I, Dienel A. (2016). Efficacy of orally administered Silexan in patients with anxiety-related restlessness and disturbed sleep – A randomized, placebo-controlled trial. European Neuropsychopharmacology, 26(2), 331–340. https://doi.org/10.1016/j.euroneuro.2015.12.002
[D25] Maia CSF. (2022). Linalool as a Therapeutic and Medicinal Tool in Depression Treatment: A Review. Current Neuropharmacology, 20(6), 1073–1092. https://doi.org/10.2174/1570159×19666210920094504
[D26] Woelk H, Schläfke S. (2010). A multi-center, double-blind, randomized study of the lavender oil preparation Silexan in comparison to lorazepam for generalized anxiety disorder. Phytomedicine, 17(2), 94–99. https://doi.org/10.1016/j.phymed.2009.10.006
Akhondzadeh S, Kashani L, Fotouhi A, et al. (2003). Comparison of Lavandula angustifolia Mill. tincture and imipramine in the treatment of mild to moderate depression: a double-blind, randomized trial. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 27(1), 123–127. https://doi.org/10.1016/S0278-5846(02)00342-1
[D28] Chen SL, Chen CH. (2015). Effects of Lavender Tea on Fatigue, Depression, and Maternal-Infant Attachment in Sleep-Disturbed Postnatal Women. Worldviews on Evidence-Based Nursing, 12(6), 370–379. https://doi.org/10.1111/wvn.12122
[D29] Navarra M, Mannucci C, Delbò M, Calapai G. (2015). Citrus bergamia essential oil: from basic research to clinical application. Frontiers in Pharmacology, 6, 36. https://doi.org/10.3389/fphar.2015.00036
[D30] Yue Y, Shen M, Xu X, et al. (2021). Antidepressant-like effects of citrus essential oil and its main component limonene in mice and rats. Journal of Agricultural and Food Chemistry, 69(12), 3555–3567. https://doi.org/10.1021/acs.jafc.0c07811
[D31] Watanabe E, Kuchta K, Kimura M, et al. (2015). Effects of bergamot (Citrus bergamia (Risso) Wright & Arn.) essential oil aromatherapy on mood states, parasympathetic nervous system activity, and salivary cortisol levels in 41 healthy females. Forschende Komplementärmedizin, 22(1), 43–49. https://doi.org/10.1159/000380989
[D32] Hieu TH, Dibas A, Surber C, et al. (2019). Therapeutic efficacy and safety of chamomile for state anxiety, generalized anxiety disorder, insomnia, and sleep quality: a systematic review and meta-analysis of randomized trials and quasi-randomized trials. Phytotherapy Research, 33(6), 1604–1615. https://doi.org/10.1002/ptr.6349
[D33] Amsterdam JD, Li QS, Xie SX, Mao JJ. (2020). Putative Antidepressant Effect of Chamomile (Matricaria chamomilla L.) Oral Extract in Subjects with Comorbid Generalized Anxiety Disorder and Depression. Journal of Alternative and Complementary Medicine, 26(9), 813–819. https://doi.org/10.1089/acm.2020.0156
[D34] Kennedy DO, Little W, Scholey AB. (2004). Attenuation of laboratory-induced stress in humans after acute administration of Melissa officinalis (Lemon Balm). Psychosomatic Medicine, 66(4), 607–613. https://doi.org/10.1097/01.psy.0000132877.72833.71
Akhondzadeh S, Noroozian M, Mohammadi M, et al. (2003). Melissa officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: a double blind, randomised, placebo controlled trial. Journal of Neurology, Neurosurgery and Psychiatry, 74(7), 863–866. https://doi.org/10.1136/jnnp.74.7.863
Moussaieff A, Rimmerman N, Bregman T, et al. (2008). Incensole acetate, an incense component, elicits psychoactivity by activating TRPV3 channels in the brain. FASEB Journal, 22(8), 3024–3034. https://doi.org/10.1096/fj.07-101865
Doğan E, Çoban A, Doğan M, et al. (2025). The effects of alpha-pinene on anxiety behaviors and TLR4/MYD88/NF-kB pathway in the hippocampus in the reserpine-induced anxiety model in rats. Acta Neuropsychiatrica. https://doi.org/10.1017/neu.2026.10080
Hongratanaworakit T, Buchbauer G. (2004). Evaluation of the harmonizing effect of ylang-ylang oil on humans after inhalation. Planta Medica, 70(7), 632–636. https://doi.org/10.1055/s-2004-827186
Choi SY, Kang P, Lee HS, Seol GH. (2014). Effects of inhalation of essential oil of Citrus aurantium L. var. amara on menopausal symptoms, stress, and estrogen in postmenopausal women: a randomized controlled trial. Evidence-Based Complementary and Alternative Medicine, 2014, 796518. https://doi.org/10.1155/2014/796518
[D40] Seol GH, Shim HS, Kim PJ, et al. (2010). Antidepressant-like effect of Salvia sclarea is explained by modulation of dopamine activities in rats. Journal of Ethnopharmacology, 130(1), 187–190. https://doi.org/10.1016/j.jep.2010.04.035
[D41] Mohebitabar S, Shirazi M, Bioos S, et al. (2017). Therapeutic efficacy of rose oil: A comprehensive review of clinical evidence. Avicenna Journal of Phytomedicine, 7(3), 206–213.
Kuroda K, Inoue N, Ito Y, et al. (2005). Sedative effects on humans of inhalation of essential oil of linalool: sensory evaluation and physiological measurements using optically active linalools. Analytica Chimica Acta, 365(1–3), 293–299. https://doi.org/10.1016/S0003-2670(98)00089-5
Kaur R, Bhardwaj A, Gupta S. (2022). Sandalwood essential oil: A review of its pharmacological properties and therapeutic uses. Natural Product Research, 36(6), 1424–1445. https://doi.org/10.1080/14786419.2021.1923765
Chomchalow N. (2001). The utilization of vetiver as medicinal and aromatic plants with special reference to Thailand. Pacific Rim Vetiver Network, Technical Bulletin No. 2001/2.
Hayashi K, Nishino H, Nishino A, et al. (2017). Cedrol, a component of wood essential oils, is a novel activator of adenylyl cyclase. Journal of Natural Products, 80(3), 846–851. https://doi.org/10.1021/acs.jnatprod.6b00841
[D46] Juergens UR, Engelen T, Racké K, et al. (2004). Inhibitory activity of 1,8-cineol (eucalyptol) on cytokine production in cultured human lymphocytes and monocytes. Pulmonary Pharmacology & Therapeutics, 17(5), 281–287. https://doi.org/10.1016/j.pupt.2004.06.002
Moss M, Cook J, Wesnes K, Duckett P. (2003). Aromas of rosemary and lavender essential oils differentially affect cognition and mood in healthy adults. International Journal of Neuroscience, 113(1), 15–38. https://doi.org/10.1080/00207450390161903
[D48] Kennedy DO, Dodd FL, Robertson BC, et al. (2011). Monoterpenoid extract of sage (Salvia officinalis) with cholinesterase inhibiting properties improves cognitive performance and mood in healthy adults. Journal of Psychopharmacology, 25(8), 1088–1100. https://doi.org/10.1177/0269881110385594
[D49] Mahboubi M. (2019). Zingiber officinale Rosc. essential oil, a review on its composition and bioactivity. Clinical Phytoscience, 5, 6. https://doi.org/10.1186/s40816-019-0097-3
Lv XN, Liu ZJ, Zhang HJ, Tzeng CM. (2012). Aromatherapy and the central nervous system (CNS): therapeutic mechanisms and their associated genes. Current Drug Targets, 13(8), 1087–1093. https://doi.org/10.2174/138945012802009092
Glossary
5-HT (5-Hydroxytryptamine / Serotonin)
Monoamine neurotransmitter; mediates mood, anxiety, sleep, appetite, and cognitive functions; often functionally deficient in depression.
5-HT1A receptor
Serotonin receptor subtype; presynaptically as an autoreceptor (feedback inhibition), postsynaptically antidepressant and anxiolytic; target of buspirone and partially of SSRIs.
alpha-Pinene
Monoterpenes from frankincense, eucalyptus, rosemary; inhibits TLR4/NF-κB signaling pathway in the hippocampus; anxiolytic and anti-neuroinflammatory.
Agomelatine
Atypical antidepressant; melatonin MT1/MT2 agonist and 5-HT2C antagonist; normalizes circadian rhythms; favorable side effect profile.
Anxiolytic
Anxiety-relieving, anxiety-reducing; an important property of many essential oils in depression-anxiety comorbidity.
Apigenin
Flavonoids from chamomile; highly selective ligand at the GABA-A benzodiazepine binding site; anxiolytic without dependence potential.
Brain-Derived Neurotrophic Factor
Neurotrophic factor; promotes neuronal survival, differentiation, and synaptic plasticity; reduced in depression; upregulated by antidepressants and terpenes.
β-Caryophyllene
Sesquiterpenes from frankincense, black pepper, cannabis; selective CB2 receptor agonist; anti-neuroinflammatory via NF-κB inhibition; relevant for the inflammatory subtype of depression.
Blood-brain barrier
Selective barrier between the bloodstream and the central nervous system; regulates the passage of substances into the brain; terpenes can bypass this via the olfactory route.
Bupropion
Dopamine-norepinephrine reuptake inhibitor (DNRI); suitable for depression with lack of drive; no sexual side effects; approved for smoking cessation.
CB2 receptor
Cannabinoid Receptor Type 2; part of the endocannabinoid system; primarily on immune cells and microglia; activation has anti-neuroinflammatory effects; target of β-caryophyllene.
cAMP/PKA/CREB cascade
Intracellular signaling pathway; activated by increased synaptic serotonin; leads to CREB phosphorylation and BDNF gene expression; common endpoint of many antidepressants.
Cedrol
Sesquiterpenes from cedarwood oil; sedative, anxiolytic; activates adenylyl cyclase; GABAergic modulation.
Cortisol
Adrenal cortex stress hormone; chronically elevated in depression (HPA hyperactivity); normalized by linalool, limonene, and other terpenes.
DAT (Dopamine Transporter)
Protein that transports dopamine from the synaptic cleft back into the nerve cell; target of bupropion and stimulants.
Dopamine-norepinephrine reuptake inhibitor
Antidepressant class that blocks DAT and NET; e.g., bupropion.
EPDS (Edinburgh Postnatal Depression Scale)
Validated screening instrument for postpartum depression; frequently used in aromatherapy studies.
GABA (gamma-aminobutyric acid)
Primary inhibitory neurotransmitter in the CNS; reduces neuronal excitability; often functionally deficient in depression and anxiety.
GABA-A receptor
Ligand-gated chloride channel; activation by GABA leads to hyperpolarization; benzodiazepine binding site is modulated by apigenin and linalool.
Generalized Anxiety Disorder (GAD)
Frequent comorbidity of depression; characterized by persistent, difficult-to-control worries; responds well to lavender and chamomile.
Geraniol
Monoterpene alcohol from rose oil, palmarosa; 5-HT1A agonism in docking studies; MAO inhibition in vitro.
HAM-D (Hamilton Depression Rating Scale)
Clinical Global Impressions-Severity scale for depression; often used as a primary endpoint in antidepressant trials.
HPA axis (Hypothalamic-Pituitary-Adrenal axis)
Neuroendocrine stress regulation system; hyperactive in depression with elevated cortisol levels; normalized by linalool and limonene.
Incensol acetate
Terpenoids from frankincense; activate TRPV3 channels; anxiolytic and antidepressant in animal models.
Linalool
Monoterpene alcohol; main active ingredient in lavender, coriander, bergamot; modulates GABA-A, 5-HT1A, HPA axis, and BDNF; best-studied antidepressant terpene.
Linalyl acetate
Linalyl ester; main component of lavender and clary sage; GABAergic and serotonergic modulation.
Limonene
Monoterpenes in citrus oils; activates 5-HT1A and Dopamine D2; normalizes HPA axis and BDNF in stress models.
MADRS (Montgomery-Åsberg Depression Rating Scale)
Validated observer-rated depression severity questionnaire; primary endpoint in the Silexan-Sertraline study.
MAO-A/B (Monoamine Oxidase A/B)
Enzymes that break down monoamines (5-HT, NA, DA); inhibition by MAOIs increases synaptic monoamine levels; also inhibited by some terpenes (eugenol, rosmarinic acid).
MAOI (Monoamine oxidase inhibitor)
Antidepressant class; irreversible (phenelzine) or reversible (moclobemide) inhibition of MAO-A/B; requires dietary restrictions with irreversible agents.
Microglia
Resident immune cells of the CNS; activated and pro-inflammatory in depression; inhibited by β-caryophyllene (CB2) and α-pinene (TLR4).
Mirtazapine
Noradrenergic and specific serotonergic antidepressant (NaSSA); blocks α2-autoreceptors and 5-HT2/5-HT3; sedating, appetite-stimulating.
Norepinephrine Transporter (NET)
Protein that transports norepinephrine from the synaptic cleft back into the nerve cell; target of SNRIs and TCAs.
Nerolidol
Sesquiterpenes from neroli, jasmine; anxiolytic in animal models; potentiates sedation.
NF-κB (Nuclear Factor kappa B)
Transcription factor; regulates pro-inflammatory genes (TNF-α, IL-6, IL-1β); elevated in depression; inhibited by β-caryophyllene, α-pinene, and other terpenes.
Neuroplasticity
Ability of the brain to adapt structurally and functionally; reduced in depression; restored by antidepressants and BDNF-promoting terpenes.
Nrf2 (Nuclear factor erythroid 2-related factor 2)
Transcription factor; master regulator of antioxidant defense; activated by terpenes (terpinen-4-ol, apigenin); reduces oxidative stress in depression.
Olfactory
Relating to the sense of smell; primary pathway of essential oils; direct access to the limbic system without crossing the blood-brain barrier.
PET (Positron Emission Tomography)
Imaging technique; uses radioactively labeled substances; enables in vivo measurement of transporter occupancy (SERT, NET, DAT) by antidepressants.
Prefrontal Cortex (PFC)
Brain region behind the forehead; important for executive functions, emotion regulation, and cognitive control; often hypofunctional in depression.
SERT (Serotonin Transporter)
Protein that transports serotonin from the synaptic cleft back into the nerve cell; primary target of SSRIs; ~80 % occupancy at therapeutic doses.
Silexan
Standardized oral lavender oil preparation (80 mg/day); the only essential oil with Phase III evidence for depression (comparable to sertraline).
SNRI (Serotonin-Norepinephrine Reuptake Inhibitor)
Antidepressant class; inhibits SERT and NET; e.g., venlafaxine, duloxetine; also effective for pain symptoms.
SSRI (Selective Serotonin Reuptake Inhibitor)
Most common antidepressant class; highly selective SERT blockade; e.g., escitalopram, sertraline, fluoxetine, paroxetine.
TCA (Tricyclic Antidepressant)
Older class of antidepressants; broad receptor profile (SERT, NET, H1, M1, α1); effective but more side effects; e.g., amitriptyline, clomipramine.
Toll-like Receptor 4 (TLR4)
Pattern recognition receptor on microglia; activates NF-κB and pro-inflammatory cascade; increased in depression; inhibited by α-pinene.
TrkB
Highly affine BDNF receptor; activation promotes neuronal survival and synaptic plasticity; common endpoint of antidepressants and neuroplasticity-promoting terpenes.
TRPV3
Thermosensitive ion channel; activated by incensole acetate (frankincense); mediates anxiolytic and antidepressant effects.
Unbounded brain concentration
Free (unbound) concentration of a substance in the brain; determines actual receptor/transporter occupancy; better predictor than total concentration.
Vetiverol / Khusimol
Sesquiterpene alcohols from vetiver oil; GABA-A modulation; anxiolytic in animal models.
1,8-Cineol (Eucalyptol)
Monoterpene oxide from eucalyptus, rosemary; AChE inhibition (cognitively enhancing); anti-neuroinflammatory via NF-κB inhibition; cognitive activation in human studies.
This report was created on April 27, 2026, based on a systematic analysis of 97 studies on antidepressant pharmacodynamics, 190 publications on essential oils in the context of depression, and 87 clinical trials. All statements are supported by primary literature.