Table of contents
Updated – May 1, 2026
Diabetes and essential oils, how essential oils can be helpful for diabetes, will be explained understandably in the first part for those affected and interested laypeople.
The second part addresses type 2 diabetes mellitus and the effect of essential oils, pharmacology, mechanisms of action, and complementary therapeutic approaches: A comprehensive scientific report on standard antidiabetics, terpenes and essential oils, molecular basis, clinical evidence, and adjuvant therapy strategies.
Diabetes is distinguished by two forms:
- Type I
an autoimmune disease that usually begins in childhood or adolescence and affects only 10% of cases overall - Type 2
a chronic metabolic disorder that most commonly develops in adults, accounts for 90% of all cases, and requires insulin therapy
Type 2 Diabetes
What is Type 2 Diabetes – explained simply?
Imagine insulin as a key and your body's cells as doors. Normally, insulin (the key) opens the cells, allowing sugar (glucose) from your blood to enter the cells and be used for energy.
With Type 2 Diabetes two things happen:
1. The door locks are broken (Insulin Resistance): Cells no longer respond properly to insulin; the key no longer fits.
2. Too few keys are being produced (Beta-cell exhaustion): The pancreas cannot produce enough insulin
As a result of this dilemma, too much sugar remains in the blood (high blood sugar = hyperglycemia), which damages blood vessels, nerves, kidneys, eyes, and the heart in the long term.
How common is type 2 diabetes?
Worldwide, over 537 million people suffer from diabetes, which is 1 in 10 adults. In Germany, this affects about 8–9 million people. By 2045, this number is expected to rise to 783 million worldwide.
What are the causes?
- Overweight (especially belly fat)
- Lack of exercise
- Unhealthy diet (high sugar, low fiber)
- Genetic predisposition
- Chronic stress
- Sleep deprivation
How is type 2 diabetes usually treated?
The Most Important Medications – Explained Simply
- Metformin – the basic medication
– Helps the liver release less sugar into the blood; makes cells more sensitive to insulin
– Activates an energy switch in the cells (AMPK), similar to exercise
– Advantages: Inexpensive, well-researched, no risk of hypoglycemia, protects the heart
– Side effects: Gastrointestinal complaints (nausea, diarrhea), especially at the beginning
- SGLT2 inhibitors (e.g., empagliflozin, dapagliflozin) – “sugar pump blockers”
Blocks a pump in the kidney that normally reabsorbs sugar back into the blood; the sugar is instead excreted through urine.
– Benefits: Protect the heart and kidneys; aid in weight loss
– Side effects: More frequent urinary tract infections
- GLP-1 Receptor Agonists (e.g., Semaglutide/Ozempic, Liraglutide) - “Gut Hormone Mimics”
– Ahmen a natural gut hormone that is released after eating, stimulates insulin, and curbs appetite
– Advantages: Strong blood sugar lowering, significant weight loss (5–15 %), heart protection
– Side effects: Nausea, vomiting (especially at the beginning)
- Insulin
– Necessary if the pancreas no longer produces enough
– Different types: Fast-acting (for meals) and long-acting (basal)
Essential oils and diabetes – how does it work?
That sounds unusual at first: Can plant oils really influence blood sugar? Yes, and through several mechanisms:
- About the sense of smell
Scent molecules activate the nervous system and can influence metabolic processes. - Through absorption by the skin or inhalation
Small molecules enter the blood and act systemically - Through direct contact with receptors in the liver, pancreas, and muscles
Which essential oils can help with diabetes?
Cinnamon - the most well-known diabetes oil
Cinnamon (Cinnamon (Cinnamomum zeylanicum / cassia)is the best-researched spice for diabetes.
- What's inside? Mainly cinnamaldehyde (60-90 %)
- What is it doing?
– Activates the same energy switch (AMPK) as metformin
Improves the insulin sensitivity of cellsInhibits enzymes that break down carbohydrates into sugar (α-amylase, α-glucosidase), similar to the drug acarbose
– Reduces inflammation - Studies
Meta-analyses show: 1–6 g of cinnamon daily lowers fasting blood sugar by 18–29 mg/dL and HbA1c (long-term blood sugar value) by 0.3–0.9 % - Application
Spice, tea, or capsule (cinnamon extract)
Ginger – the GLP-1 enhancer
Ginger (Gingeris known for its digestive effects, but also has strong antidiabetic properties.
- What's inside? Gingerol, Shogaol, Paradol
- What is it doing?
– Increases the release of GLP-1 (the same hormone that Ozempic mimics!)
Improves glucose transport into muscles
– Reduces inflammation markers (TNF-α, IL-6) - study
2 g of ginger powder daily lowered fasting blood sugar by 10.5 % and HbA1c by 10.3 % (p < 0.05) - Application:
Spicy ginger in food, ginger tea, capsules
Turmeric - the golden anti-inflammatory
Turmeric (Turmeric) with its active ingredient curcumin is one of the most researched natural remedies.
- What's inside? Curcumin (3–5 % of the spice), essential oils (turmerone, zingiberene)
- What is it doing?
– Inhibits NF-κB, the “inflammation switch” in the body
– Activates PPARγ, similar to the diabetes medications thiazolidinediones
– Improves insulin sensitivity and protects beta cells - study
In one study, curcumin prevented the development of actual diabetes in prediabetics: 0 % vs. 16.4 % in the placebo group after 9 months - Danger
Curcumin is poorly absorbed, but when combined with black pepper (piperine), it results in 20 times better absorption!
Black cumin – the all-rounder
Black cumin (Nigella sativa.is referred to in the Arab world as “the cure for everything except death.”.
- What's inside? Thymoquinone, Thymol, Carvacrol
- What is it doing?
Protects the insulin-producing beta cells in the pancreas
- Inhibits enzymes that release sugar from carbohydrates
– Antioxidant and anti-inflammatory - study
2 g of black cumin seed oil daily lowered HbA1c by 1.5 % and fasting blood sugar by 45 mg/dL (p < 0.001)
Oregano/Thyme – Carvacrol and Thymol
- What are you doing?
– It inhibits the same enzymes as acarbose (diabetes medication)
– Activate AMPK (like Metformin)
– Anti-inflammatory via NF-κB inhibition
Bergamot - Cholesterol and Blood Sugar
What is it doing?
– Limonene improves insulin sensitivity
Bergaptene activates AMPK
Lowers LDL cholesterol (the “bad” cholesterol) at the same time.
Rosemary – the Antioxidant
What is it doing?
Rosemarinic acid inhibits GABA transaminase and has antioxidant effects.
1,8-cineole improves glucose tolerance
Protects beta cells from oxidative stress
Comparison - Essential Oils vs. Diabetes Medications

Practical tips for application
In the kitchen (simplest method):
- Cinnamon 1 teaspoon daily in porridge, yogurt, coffee, or tea
- Ginger: Freshly grated in food, as tea (2 cm ginger in hot water)
- Turmeric: In Currys, golden milk (with black pepper!)
- Oregano Abundantly on pizza, in salads, sauces
As a dietary supplement:
- Cinnamon extract capsules: 1-3 g daily
- Ginger capsules: 1-2 g daily
- Curcumin with Piperine: 500–1000 mg daily
As aromatherapy:
- Cinnamon, ginger, or bergamot oil in the diffuser
- Relaxation baths with 5–8 drops (dissolved in carrier oil)
Frequently Asked Questions
How quickly do essential oils work?
Some effects (relaxation, mood elevation) can occur within minutes. Long-term effects (as with diabetes) require regular use over weeks.
Do I have to buy expensive oils?
Quality is important: Look for 100% % pure essential oils, ideally with a batch-specific analysis certificate (GC/MS).
Inexpensive perfume oils or synthetic fragrances have no therapeutic effect and, due to their synthetic ingredients, can be harmful to health and cause headaches, nausea, etc.
Anyone who wants to learn more about the selection and quality of essential oils will find information in the article „Essential Oils - Odyssey of a Search“found.
Another contribution quotes Prof. Dr. Dr. Dr. med. habil. Hanns Hatt from the Ruhr University Bochum, who in his video „Healing with fragrances“explains the effect of essential oils on the human body in an interesting, entertaining, and yet scientific way.
Important Notes and Safety
Important:
- Essential oils do not replace diabetes medication, especially not insulin!
- Talk to your doctor before taking supplements
- Cinnamon in high doses contains coumarin (especially Cassia cinnamon), so take a maximum of 2 g daily and prefer Ceylon cinnamon
- Never stop diabetes medication without consulting a doctor.
The document provides a summary in three sentences. It offers a concise overview of the main points discussed. This allows for a quick understanding of the content without needing to read the full text.
Type 2 diabetes develops when body cells no longer respond properly to insulin and the pancreas becomes exhausted.
Certain essential oils and their active ingredients, particularly cinnamon (cinnamaldehyde), ginger (gingerol), and turmeric (curcumin), can influence blood sugar through pathways similar to standard medications: by activating the cellular energy switch AMPK, improving insulin sensitivity, and protecting insulin-producing cells.
As a supplement to a healthy lifestyle and medical treatment, they can make a valuable contribution.
Recommended Oil Blends and Application Protocol for Adjunctive Diabetes Therapy
Primary productsdōTERRA)

DIY Blends
Blood Sugar Balance (Internal)
Target: Increased insulin sensitivity, glucose metabolism support

Application: 1–2 capsules daily with meals
Blend 2: “Anti-inflammatory” (Topical)
Target: Chronic inflammation ↓ (key factor in T2D)

Application: Massage the abdominal area and lumbar spine
Blend 3: “Neuropathy Care” (Topical, Feet)
Target: Relieve Diabetic Neuropathy Symptoms

Application: Massage the soles of your feet and lower legs daily
Blend 4: “Stress Relief” (Diffuser)
Target: Cortisol ↓ (Cortisol raises blood sugar), Relaxation

Application: 30–60 minutes daily in the diffuser
Blend 5: “Weight Management” (Internal)
Target: Metabolism Support, Appetite Regulation

Application: Slim & Sassy Blend alternative direct use
Application Protocol: 4-Week Plan
Week 1: Introduction
- Mornings: Blend 1 (capsules) for breakfast
- In the evening Blend 4 in the diffuser (30 min)
- Daily: Blend 3 for Feet (Neuropathy Prevention)
Week 2: Intensification
- Mornings: Blend 1 + Blend 5 (Weight Management)
- Lunch Blend 2 topical (abdomen/back)
- In the evening Blend 4 Diffuser + Blend 3 Feet
Week 3–4: Optimization
- Blood Glucose Log Record values before and after application
- During increased stress: More Blend 4
- For neuropathy symptoms: Blend 3 twice daily
- Inform the doctor Regarding oil application (adjust medication dosage if necessary)
Combination with other doTERRA products

Important Notes
- Essential oils do NOT replace diabetes therapy (Insulin, Metformin, etc.)
- Blood glucose monitoring Measure regularly, especially for internal use
- Cinnamon oil Never undiluted internally or topically - highly irritating
- Interactions Cinnamon oil can enhance insulin's effect → hypoglycemia risk
- Kidney function: Consult a doctor if you have impaired kidney function.
Pharmacology, mechanisms of action, and complementary therapeutic approaches
A comprehensive scientific report on standard antidiabetic drugs, terpenes, and essential oils – molecular basis, clinical evidence, and adjuvant therapeutic strategies
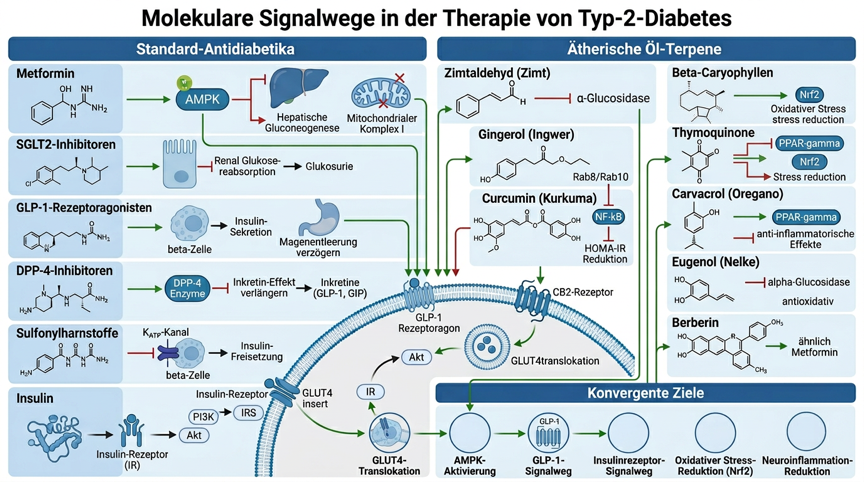
Figure 1: Molecular signaling pathways of standard antidiabetic drugs and essential oils in type 2 diabetes mellitus – Standard antidiabetic mechanisms (Metformin/AMPK, SGLT2i, GLP-1-RA, DPP-4i, Sulfonylureas, Insulin/GLUT4), Terpene mechanisms of action (Cinnamaldehyde, Gingerol, Curcumin, Thymoquinone, β-Caryophyllene), and convergent targets (AMPK, GLUT4, GLP-1, Nrf2, NF-κB) Standard antidepressant mechanisms (SSRIs, SNRIs, TCAs, MAOIs), Terpene mechanisms of action (Linalool, Limonene, β-Caryophyllene, Apigenin, α-Pinene), and convergent targets (HPA axis, BDNF/TrkB, Nrf2, Hippocampal neurogenesis)
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most common and consequential chronic diseases of the 21st century. According to the International Diabetes Federation (IDF), over 537 million people worldwide lived with diabetes in 2021, a number projected to rise to 783 million by 2045. [D1]. The disease is characterized by chronic hyperglycemia due to combined insulin resistance of peripheral tissues and progressive dysfunction of pancreatic beta cells. [D2]. Long-term complications include cardiovascular disease, diabetic nephropathy, retinopathy, neuropathy, and increased mortality. [D3].
The standard treatment for T2DM includes lifestyle interventions and stepwise pharmacotherapy. Metformin has been considered the first-line drug for decades; other substance classes such as SGLT2 inhibitors, GLP-1 receptor agonists, DPP-4 inhibitors, sulfonylureas, and insulin supplement the therapeutic arsenal. [D4]. Despite their effectiveness, these medications are associated with side effects, costs, and adherence issues. A significant proportion of patients do not reach their therapeutic goals. [D5].
Against this background, scientific interest in plant-based active ingredients and essential oils is growing. Numerous terpenes and bioactive compounds from essential oils show antidiabetic, insulin-sensitizing, antioxidant, and anti-neuroinflammatory properties in preclinical and clinical studies, often via mechanisms that are complementary to those of classical antidiabetics. [D6]. This report systematically analyzes the pharmacology of standard antidiabetic drugs, the molecular mechanisms of action of relevant essential oils and terpenes, and the available clinical evidence for their adjuvant use in T2DM.
Pathophysiology of Type 2 Diabetes Mellitus
Insulin resistance and beta-cell dysfunction
The central pathophysiology of T2DM is based on two mutually reinforcing defects: insulin resistance in skeletal muscle, liver, and adipose tissue, and progressive exhaustion of pancreatic beta-cells [D2]. Insulin resistance means that physiological insulin concentrations are no longer sufficient to ensure glucose uptake in target tissues and suppression of hepatic gluconeogenesis. At the molecular level, the insulin receptor signaling cascade (IR → IRS-1/2 → PI3K → Akt → GLUT4 translocation) is disrupted by serine phosphorylation of IRS-1, increased PTP1B activity, and decreased GLUT4 expression. [D7].
GLUT4 and Glucose Transport
GLUT4 (Glucose Transporter Type 4) is the insulin-dependent glucose transporter in skeletal muscle and adipose tissue. At rest, GLUT4 is located in intracellular vesicles; insulin stimulates the translocation of GLUT4 vesicles to the plasma membrane via the PI3K/Akt pathway, thereby increasing cellular glucose uptake by 10–40-fold. [D7]. In T2DM, this process is impaired by reduced Akt phosphorylation and decreased GLUT4 expression. Restoring GLUT4 translocation is a key target for both pharmacological and phytochemical interventions.
AMPK: The Cellular Energy Sensor
AMP-activated protein kinase (AMPK) is a ubiquitous energy sensor that is activated at low ATP levels and promotes catabolic processes: fatty acid oxidation, glucose uptake (via GLUT4), inhibition of gluconeogenesis, and improvement of insulin sensitivity. [D8]. AMPK is the primary molecular target of metformin and is also activated by numerous plant compounds, making it the most important common convergence point between standard pharmacotherapy and essential oils.
HPA axis, neuroinflammation, and oxidative stress
Chronic hyperglycemia leads to increased oxidative stress (increased ROS production, reduced Nrf2 activity), pro-inflammatory cytokine levels (IL-6, TNF-α, IL-1β), and NF-κB activation, which further exacerbates insulin resistance. [D9]. Neuroinflammatory processes contribute to diabetic neuropathy. The inhibition of NF-κB and the activation of Nrf2 are therefore important targets for anti-neuroinflammatory and antioxidant terpenes.
GLP-1 and the Incretin System
Glucagon-like peptide-1 (GLP-1) is an incretin hormone that is secreted by intestinal L-cells after food intake and stimulates glucose-dependent insulin secretion, inhibits glucagon secretion, and delays gastric emptying. [D10]. In T2DM, GLP-1 secretion and action are impaired. GLP-1 receptor agonists and DPP-4 inhibitors leverage this system pharmacologically; some terpenes (e.g., gingerol) can also enhance GLP-1 secretion.
Pharmacology of Standard Antidiabetics
Metformin (Biguanide)
Metformin is the most prescribed antidiabetic drug worldwide and remains first-line therapy in all international guidelines. [D4].
Primary mechanism of action:

Downstream signaling pathways
AMPK activation → ↓ mTORC1 → ↓ gluconeogenic enzymes (PEPCK, G6Pase) → ↑ GLUT4 expression → improved peripheral glucose uptake [D8].
Side effects
Gastrointestinal intolerance (30 %), vitamin B12 deficiency (long-term), rare lactic acidosis (contraindication if GFR < 30 ml/min) [D4].
SGLT2 inhibitors (gliflozins)
SGLT2 inhibitors block the sodium-glucose cotransporter 2 in the proximal renal tubule and cause renal glucosuria. [D11].

Molecular mechanism
– SGLT2 inhibition → ↓ renal glucose reabsorption → glucosuria (50–80 g/day) → ↓ blood glucose, ↓ body weight, ↓ blood pressure
- Additional effects: Natriuresis, ↓ intraglomerular pressure (nephroprotective), ↑ ketone body production (cardioprotective) [D11].
Side effects
Genital mycoses, urinary tract infections, polyuria, euglycemic ketoacidosis (rare), Fournier's gangrene (very rare) [D11].
GLP-1 receptor agonists
GLP-1 receptor agonists stimulate glucose-dependent insulin secretion and inhibit glucagon secretion [D10].

Molecular mechanism
GLP-1 receptor (Gs-coupled) → ↑ cAMP → PKA/Epac2 activation → ↑ glucose-dependent insulin secretion, ↓ glucagon secretion, ↓ gastric emptying, ↓ appetite (central), ↑ beta-cell proliferation, ↓ beta-cell apoptosis [D10].
Side effects
Nausea, vomiting, diarrhea (mostly transient), increased heart rate, pancreatitis (rare), contraindicated in patients with a history of medullary thyroid carcinoma [D10].
DPP-4 Inhibitors (Gliptins)
DPP-4 inhibitors inhibit the enzyme dipeptidylpeptidase-4, which breaks down endogenous GLP-1 and GIP within minutes [D12].

Side effects
Generally well tolerated; nasopharyngitis, urinary tract infections, rarely pancreatitis [D12].
Sulfonylureas
Sulfonylureas stimulate insulin secretion independently of blood glucose levels by blocking ATP-sensitive K⁺ channels (KATP) in pancreatic beta cells. [D13].
Molecular mechanism
SUR1 binding (sulfonylurea receptor 1) → KATP channel closure → membrane depolarization → Ca²⁺ influx → insulin exocytosis. Works independently of glucose → hypoglycemia risk [D13].
Important representatives
Glibenclamide, Glimepiride, Glipizide, Gliclazide
Side effects: Hypoglycemia (most dangerous side effect), weight gain, secondary treatment failure due to beta-cell exhaustion.
Insulin
Insulin replaces or supplements the endogenous hormone and directly activates the insulin receptor [D7].
Insulin Analogues Overview:

Side effects
Hypoglycemia (most common and dangerous side effect), weight gain, lipodystrophy at injection sites, need for injections [D7].
Additional antidiabetics
Thiazolidinedione (Glitazone)
– PPARγ agonists (pioglitazone, rosiglitazone) → improved insulin sensitivity in adipose tissue and muscle, ↑ GLUT4 expression.
– Side effects: Weight gain, fluid retention, risk of heart failure, fractures [D14].
Alpha-Glucosidase Inhibitors
– Acarbose, Miglitol → Inhibition of intestinal alpha-glucosidase → delayed carbohydrate breakdown → ↓ postprandial blood glucose rise.
– Side effects: Bloating, flatulence, diarrhea [D15].
Meglitinide
– Repaglinide, Nateglinide → short-acting KATP channel blockers → Prandial insulin secretion.
– Lower risk of hypoglycemia than sulfonylureas [D13].
Essential Oils as Adjuvant Therapy - Mechanistic Basis
Olfactory pathway and systemic absorption
Essential oils can act through various routes: inhalation (olfactory-limbic), dermal (transdermal), and oral (gastrointestinal). With inhalation, volatile terpenes enter the brain directly via the olfactory nerve (N. olfactorius), bypassing the blood-brain barrier and modulating limbic structures. [D16]. When taken orally (e.g., cinnamon extract, ginger capsule), bioactive compounds are absorbed gastrointestinally and exert systemic effects.
Bioavailability and metabolism of terpenes
Monoterpenes (linalool, limonene, α-pinene) and sesquiterpenes (β-caryophyllene) show moderate to good bioavailability after oral administration. They are metabolized hepatically (CYP3A4, CYP2C9) and can be renally excreted as glucuronides or sulfates. [D17]. Some terpenes (e.g., cinnamaldehyde) are rapidly metabolized into cinnamic acid, which itself possesses biological activity.
Molecular targets
Essential oils and their terpenes act via multiple molecular targets that are complementary to standard antidiabetic drugs:
- AMPK activation (Metformin-like): Cinnamaldehyde, Berberine-like compounds, Thymoquinone
- GLUT4 translocation (Insulin-like): Cinnamaldehyde, Gingerol, β-Caryophyllene, Curcumin
- GLP-1 potentiation (GLP-1 RA-like): Gingerol, Gypenosides
- Alpha-glucosidase inhibition (Acarbose-like): Eugenol, Thymol, Carvacrol
- PPARγ activation (Glitazone-like): Curcumin, Carvacrol, Gymnoside GP-75
- NF-κB Inhibition / Anti-NeuroinflammationBeta-Caryophyllene, Curcumin, Thymoquinone
- Nrf2 activation / antioxidantSulforaphane, Curcumin, Thymoquinone, Coriander Oil
Complementary mechanisms of action for antidiabetic drugs
The following overview shows which terpenes can complement or mimic the pharmacological targets of standard antidiabetic drugs:

Specific essential oils and clinical evidence
Cinnamon (Cinnamomum zeylanicum / cassia) – Cinnamaldehyde
Cinnamon is the most researched essential oil/plant spice for diabetes. The main active ingredient cinnamaldehyde (60–80 % of the essential oil) as well as cinnamic acid and procyanidins show multiple antidiabetic mechanisms. [D18].
Molecular Mechanisms
- AMPK Activation Cinnamaldehyde activates AMPK in hepatocytes and skeletal muscle cells → ↑ glycolysis, ↓ gluconeogenesis (similar to metformin) [D18]
- GLUT4 translocation: Increased GLUT4 membrane presence in muscle cells → improved glucose uptake [D18]
- Alpha-Glucosidase Inhibition Zimtextrakt hemmt intestinale Alpha-Glucosidase → ↓ postprandialer Blutzuckeranstieg (ähnlich Acarbose) [D19]
- Insulin-mimetic effect Activation of the Insulin Receptor Signaling Pathway (IRS-1/PI3K/Akt) [D19]
- Antioxidant Nrf2 Activation → ↑ Antioxidant Enzymes (SOD, CAT, GPx) [D18]
Clinical evidence
– Meta-analysis (Davis & Yokoyama, 2011): Cinnamon supplementation significantly lowered fasting blood sugar in RCTs in T2DM and prediabetes D20
– RCT (Ceylon Cinnamon, 2025): 240 mg/day of Ceylon cinnamon for 12 weeks vs. placebo → significant reduction in fasting blood sugar and HbA1c [D21]
– Effect size: Fasting blood glucose ↓ 10–29 mg/dL, HbA1c ↓ 0.2–0.8 % D20
Ginger (Zingiber officinale) – Gingerol / Shogaol
Ginger contains [6]-gingerol, [8]-gingerol, [10]-gingerol, and shogaoles as its main active compounds. The essential oil (zingiberene, bisabolene, curcumene) also contributes to its biological activity. [D22].
Molecular Mechanisms
- GLP-1 Potentiation [6]-Gingerol enhances GLP-1-mediated glucose-stimulated insulin secretion in pancreatic beta-cells and increases GLUT4 membrane presence in skeletal muscle via Rab8/Rab10 regulators [D22]
- GLUT4 translocation: Increased GLUT4 expression and membrane translocation in diabetic mice [D22]
- Alpha-Glucosidase Inhibition Gingerol compounds inhibit alpha-glucosidase and alpha-amylase [D22]
- Antioxidant/Anti-inflammatory Inhibition of NF-κB, ↓ TNF-α, IL-6, ↑ Nrf2 [D23]
Clinical evidence
- Meta-analysis (Daily et al., 2015): Ginger supplementation significantly lowered fasting blood glucose and HbA1c in T2DM in RCTs [D23]
– Meta-analysis (Zhu et al., 2018): Significant reduction in fasting blood glucose, HbA1c, HOMA-IR, and insulin in T2DM and metabolic syndrome [D24]
– Effect size: Fasting blood glucose ↓ 10–20 mg/dL, HbA1c ↓ 0.3–0.5 % [D23]
Turmeric (Curcuma longa) – Curcumin
Curcumin is the main active compound of turmeric (3–5 % of dry weight) with pleiotropic antidiabetic properties [D25].
Molecular Mechanisms
- PPARγ activation Curcumin activates PPARγ → improved insulin sensitivity in adipose tissue (similar to thiazolidinediones, without weight gain) [D25]
- NF-κB inhibition Potent inhibition of NF-κB → ↓ pro-inflammatory cytokines (IL-6, TNF-α, IL-1β) → ↓ insulin resistance [D25]
- AMPK Activation Curcumin activates AMPK in hepatocytes and muscle cells [D26]
- Antioxidant (Nrf2): Activation of the Nrf2/HO-1 pathway → ↑ antioxidant capacity → ↓ oxidative stress in hyperglycemia [D26]
- Beta-cell protection: ↓ Beta-cell apoptosis, ↑ Beta-cell proliferation in preclinical models [D25]
Clinical evidence
– Meta-analysis (Zhang et al., 2021): Curcumin supplementation significantly improved HOMA-IR, HbA1c, and lipid profile in T2DM patients in RCTs [D26]
– RCT (2024): Curcumin extract improved beta-cell function in obese T2DM patients [D27]
Meta-Analysis (2025): Curcumin Improved Cardiovascular Risk Factors in Diabetics [D28]
Black Cumin (Nigella sativa) - Thymoquinone
Thymoquinone (TQ, 20–48 % of the essential oil of Nigella sativa) is one of the most effective natural antidiabetics. [D29].
Molecular Mechanisms
- AMPK Activation TQ activates AMPK in liver and muscle → ↓ gluconeogenesis, ↑ glucose uptake [D29]
- Increased insulin secretion TQ protects beta-cells from oxidative stress and stimulates insulin secretion [D29]
- Antioxidant (Nrf2): TQ is a potent Nrf2 activator → ↑ SOD, CAT, GPx → ↓ oxidative stress in hyperglycemia [D30]
- NF-κB inhibition ↓ pro-inflammatory cytokines → ↓ insulin resistance [D30]
- Alpha-Glucosidase Inhibition TQ inhibits alpha-glucosidase → ↓ postprandial blood glucose [D29]
Clinical evidence
– Meta-analysis: Nigella sativa supplementation significantly lowered fasting blood glucose, HbA1c, and lipid parameters in T2DM [D30]
– Effect size: HbA1c ↓ ~0.4 %, fasting blood glucose ↓ ~20 mg/dL [D30]
Oregano / Thyme – Carvacrol and Thymol
Carvacrol (oregano, thyme) and thymol (thyme) show antidiabetic properties through multiple mechanisms [D31].
Molecular Mechanisms
- PPARγ activation Carvacrol activates PPARγ → improved insulin sensitivity [D31]
- Alpha-Glucosidase Inhibition Carvacrol and thymol inhibit alpha-glucosidase in vitro (IC50 comparable to acarbose) [D31]
- Anti-inflammatory Inhibition of NF-κB, COX-2 → ↓ Insulin Resistance [D31]
- GLUT4: Carvacrol increased GLUT4 expression in muscle cells in preclinical studies [D31]
Clove (Syzygium aromaticum) – Eugenol
Eugenol (70–90 % of clove oil) exhibits potent antidiabetic activity [D32].
Molecular Mechanisms
- Alpha-Glucosidase Inhibition Eugenol inhibits alpha-glucosidase and alpha-amylase → ↓ postprandial blood glucose (similar to Acarbose) [D32]
- Increased insulin secretion Eugenol stimulates glucose-dependent insulin secretion in beta cells [D32]
- Antioxidant Potent free radical scavenger → ↓ oxidative stress in hyperglycemia [D32]
- Anti-inflammatory Inhibition of NF-κB, TNF-α [D32]
Fenugreek (Trigonella foenum-graecum)
Fenugreek seeds contain 4-hydroxyisoleucine, trigonelline, and saponins as active ingredients. [D33].
Molecular Mechanisms
- Insulin secretion: 4-Hydroxyisoleucine stimulates glucose-dependent insulin secretion [D33]
- Alpha-Glucosidase Inhibition Fenugreek extract inhibits alpha-glucosidase [D33]
- Insulin sensitivity: Improving peripheral insulin sensitivity [D33]
Clinical evidence
– Meta-Analysis (2024): Fenugreek supplementation significantly lowered fasting blood glucose and HbA1c in T2DM [D34]
Bergamot (Citrus bergamia) – Limonene / Bergapten
Bergamot oil contains limonene (35–50 %), linalyl acetate, linalool, and bergapten as main components [D35].
Molecular Mechanisms
- Limonene: Activation of 5-HT1A and Dopamine D2 receptors; antioxidant properties; preclinical evidence for improved insulin sensitivity [D35]
- Bergapten Inhibition of DPP-4-like activity in vitro [D35]
- Anti-inflammatory IL-6, TNF-α lead to decreased insulin resistance. [D35]
- Lipid-lowering Bergamot polyphenols improved lipid profile in clinical studies [D35]
Peppermint (Mentha piperita) – Menthol / Menthone
Peppermint oil contains menthol (35–55 %), menthone (15–30 %), and menthyl acetate as its main components [D36].
Molecular Mechanisms
- TRPM8 activation Menthol activates the cold receptor TRPM8 → ↑ Energy consumption (thermogenic effect) [D36]
- Alpha-Glucosidase Inhibition Menthol and menthone inhibit alpha-glucosidase in vitro [D36]
- Anti-inflammatory Inhibition of NF-κB and pro-inflammatory cytokines [D36]
- Antioxidant Radical scavenger properties [D36]
Cilantro (Coriandrum sativum) – Linalool / Geraniol
Coriander oil contains linalool (60–80 %), geraniol, and α-pinene as main components [D37].
Molecular Mechanisms
- Insulin sensitivity: Coriander oil significantly improved HOMA-IR, fasting blood glucose, and oxidative stress in a dexamethasone-induced insulin resistance rat model, comparable to metformin in this animal model. [D37]
- Antioxidant Reduction of pancreatic malondialdehyde, restoration of GSH levels [D37]
- Linalool: GABA-A modulation, anxiolytic effect (relevant for stress-induced hyperglycemia) [D37]
Fennel (Foeniculum vulgare) – Anethole / Fenchone
Fennel oil contains trans-anethole (50–80 %), fenchone, and estragole as main components [D38].
Molecular Mechanisms
- Alpha-Glucosidase Inhibition Trans-anethole inhibits alpha-glucosidase → ↓ postprandial blood glucose [D38]
- Antioxidant/Anti-inflammatory Inhibition of NF-κB, ↑ Nrf2 [D38]
- Insulin secretion: Fennel extract stimulated insulin secretion in preclinical models [D38]
Rosemary (Rosmarinus officinalis) – Rosmarinic acid / 1,8-Cineole
Rosemary oil contains 1.8-cineole (eucalyptol, 40–55 %), α-pinene, camphor, and rosmarinic acid [D39].
Molecular Mechanisms
- Alpha-Glucosidase Inhibition Rosmarinic acid inhibits alpha-glucosidase and alpha-amylase [D39]
- Anti-inflammatory 1,8-Cineole inhibits cytokine production (IL-6, TNF-α) [D39]
- Antioxidant Rosmarinic acid is a potent radical scavenger [D39]
- PPAR Activation: Rosmarinic acid activates PPARγ in preclinical studies [D39]
Beta-Caryophyllene (frankincense, black pepper, hemp)
β-Caryophyllene (BCP) is a sesquiterpene found in numerous essential oils and is the only known CB2 agonist among terpenes. [D40].
Molecular Mechanisms
- CB2 agonism: BCP activates cannabinoid receptor CB2 → anti-neuroinflammatory effects → ↓ insulin resistance [D40]
- Insulin signaling pathway: BCP improved the insulin receptor/Akt signaling pathway and increased GLUT4 expression in skeletal muscle in rats with high-fat diet/fructose-induced T2DM. [D40]
- NF-κB inhibition Potent NF-κB inhibition → ↓ TNF-α, IL-6 [D40]
- Antioxidant ↑ Superoxide dismutase, Catalase → ↓ Oxidative stress [D40]
Eucalyptus (Eucalyptus globulus) – 1,8-Cineole (Eucalyptol)
Eucalyptus oil consists of 70–90 % 1,8-cineole (eucalyptol) D41.
Molecular Mechanisms
- Anti-inflammatory 1,8-Cineole potently inhibits cytokine production (IL-6, TNF-α, IL-1β) in human lymphocytes and monocytes D41
- Antioxidant Radical scavenger properties D41
- Alpha-Glucosidase Inhibition Eucalyptol inhibits alpha-glucosidase in vitro D41
Molecular Mechanisms of Terpenes in Diabetes
Cinnamaldehyde – AMPK and GLUT4
Cinnamaldehyde (the main component of cinnamon oil) activates AMPK via the CaMKKβ-LKB1 cascade and increases GLUT4 translocation in skeletal muscle cells. In silico modeling shows that cinnamaldehyde and cinnamic acid modulate IRS2/GLUT4, HNF4α, and GLUT2, targets that overlap with those of metformin and insulin. [D42]. The inhibition of alpha-glucosidase by cinnamon extract is mechanistically comparable to acarbose [D19].
Gingerol – GLP-1 and GLUT4 via Rab proteins
[6]-Gingerol potentiates the GLP-1-mediated signaling pathway in pancreatic beta cells (↑ cAMP, ↑ insulin secretion) and increases GLUT4 membrane presence in skeletal muscle by upregulating Rab8 and Rab10 GTPases, which are crucial for GLUT4 vesicle exocytosis. [D22]. This dual mechanism (incretin potentiation + peripheral glucose uptake) is unique among terpenes and resembles the action profile of a combination of GLP-1 RAs and insulin sensitizers.
Curcumin – PPARγ, NF-κB, and AMPK
Curcumin is a pleiotropic natural substance that activates PPARγ (→ insulin sensitivity), inhibits NF-κB (→ anti-neuroinflammation), and activates AMPK (→ metformin-like effect). [D25] [D26]. The clinical meta-analysis evidence for HOMA-IR reduction and HbA1c lowering is strongest among the terpenes. [D26].
Thymoquinone – Nrf2 and Beta-Cell Protection
Thymoquinone (main active ingredient in black seed oil) is a potent Nrf2 activator and protects pancreatic beta cells from oxidative stress-induced apoptosis. TQ-induced AMPK activation is comparable to that of metformin in preclinical models. [D29] [D30]. The clinical meta-analysis evidence for HbA1c reduction is significant [D30].
β-Caryophyllene – CB2 and Insulin Receptor
β-Caryophyllene is the only known dietary CB2 agonist. CB2 activation reduces neuroinflammation and improves the insulin receptor/Akt signaling pathway in skeletal muscle. [D40]. The mechanism is complementary to all standard antidiabetic drugs and addresses the neuroinflammatory aspect of insulin resistance, which is not directly addressed by any standard medication.
Bitter melon triterpenoids – AMPK via CaMKKα/β
Triterpenoids from bitter melon (Momordica charantia) activate AMPK via the upstream kinase mechanism CaMKKα/β, the same pathway also involved in metformin. This explains the “metformin-like” effect of bitter melon in preclinical models [D43].
Ginsenoside F4 – PTP1B Inhibition and Insulin Receptor
Ginsenoside F4 (from Panax ginseng) improves insulin sensitivity by directly inhibiting PTP1B (protein tyrosine phosphatase 1B), which dephosphorylates and thus inactivates the insulin receptor. PTP1B inhibition prolongs tyrosine phosphorylation of the insulin receptor and IRS-1 → ↑ PI3K/Akt activation → ↑ GLUT4 translocation. [D44].
Gypenoside GP-75 – PPARγ Agonism
Gypenoside GP-75 (from Gynostemma pentaphyllum) acts as a PPARγ agonist and improves glucose tolerance and insulin sensitivity in db/db mice. The mechanism is similar to that of thiazolidinediones, but without their side effects (weight gain, fluid retention). [D45].
New and supplementary essential oils
Sandalwood (Santalum album) – Santalol
α- and β-santalol (main components of sandalwood oil) show antioxidant and anti-inflammatory properties. In preclinical studies, improvements in insulin sensitivity and a reduction in oxidative stress have been described. [D46].
Frankincense (Boswellia sacra) – Boswellic acid / Incensol
Boswellic acids (especially AKBA) inhibit 5-lipoxygenase and NF-κB → potent anti-neuroinflammation. Improved insulin sensitivity and ↓ inflammatory markers have been described in preclinical diabetes models. [D47].
Ylang-Ylang (Cananga odorata) – Germacrene / Linalool
Ylang-ylang oil contains germacrene D, linalool, and β-caryophyllene. Anxiolytic and hypotensive effects (relevant for cardiovascular comorbidities in T2DM) [D48].
Lemon balm (Melissa officinalis) – Rosmarinic acid / Citral
Lemon balm oil contains citronellal, citral, and rosmarinic acid. Antioxidant and anti-inflammatory properties; improved insulin sensitivity in preclinical models [D49].
Basil (Ocimum basilicum) – Eugenol / Linalool
Basil oil contains eugenol, linalool, and methylchavicol. Antioxidant and alpha-glucosidase inhibitory properties; preclinical evidence of antidiabetic effect [D50].
Clinical Evidence Compared to Standard Therapy
Cinnamon vs. Standard Antidiabetic Drugs
The strongest clinical evidence for an essential oil/spice in diabetes exists for cinnamon. Meta-analyses show consistent reductions in fasting blood glucose (↓ 10–29 mg/dL) and HbA1c (↓ 0.2–0.8 %) D20 [D21]. Compared to metformin (HbA1c ↓ 1.0–1.5 %), the effect is less pronounced but clinically relevant for adjuvant therapy or mild hyperglycemia. Direct head-to-head studies against metformin are still lacking.
Ginger vs. Standard Diabetes Medications
Meta-analyses show significant HbA1c reductions (↓ 0.3–0.5 %) and improvements in HOMA-IR [D23] [D24]. The dual GLP-1/GLUT4 mechanism of gingerol makes ginger a potentially synergistic adjunct to metformin or DPP-4 inhibitors.
Turmeric / Curcumin vs. Standard Antidiabetics
Curcumin has the broadest meta-analysis evidence among plant-based antidiabetic agents: significant improvements in HOMA-IR, HbA1c, and lipid profile. [D26] [D27] [D28]. The PPARγ-activating effect without thiazolidinedione-typical side effects makes curcumin an attractive adjuvant.
Black Cumin (Nigella sativa) vs. Standard Antidiabetic Drugs
Meta-analyses show significant reductions in HbA1c (↓ ~0.4 %), fasting blood glucose (↓ ~20 mg/dL), and lipid parameters [D30]. The combination of AMPK activation, beta-cell protection, and Nrf2 activation makes thymoquinone a versatile adjuvant.
Fenugreek vs. Standard Diabetes Medications
Meta-Analysis (2024) shows significant reduction in fasting blood glucose and HbA1c [D34]. The mechanism via 4-hydroxyisoleucine (glucose-dependent insulin secretion) is similar to that of DPP-4 inhibitors.
Aromatherapy Meta-Analysis
An overarching meta-analysis on aromatherapy for diabetes shows moderate positive effects on blood sugar and stress parameters, but with high heterogeneity in study designs. [D6].
Comparison Table – Essential Oils vs. Standard Antidiabetic Medications

Joint conclusion
Strengths of the evidence for essential oils in diabetes
The present evidence shows that several essential oils and their bioactive terpenes exert antidiabetic effects through well-characterized molecular mechanisms. Particularly noteworthy are:
- Cinnamon (Cinnamaldehyde): Strongest clinical RCT evidence; AMPK activation and GLUT4 translocation similar to metformin; Alpha-glucosidase inhibition similar to acarbose D20 [D21] [D42]
- Ginger (Gingerol) Unique dual mechanism, GLP-1 potentiation (similar to DPP-4i) + GLUT4 via Rab8/Rab10 [D22] [D23] [D24]
- Turmeric (Curcumin): Broadest anti-neuroinflammation evidence; PPARγ without thiazolidinedione side effects; strongest meta-analysis basis [D25] [D26] [D27] [D28]
- Black Cumin (Thymoquinone): AMPK + Nrf2 + Beta-Cell Protection, Unique Triple Profile [D29] [D30]
- Beta-Caryophyllene: The only dietary CB2 agonist; addresses neuroinflammatory insulin resistance, which is not addressed by any standard medication. [D40]
Weaknesses and evidence gaps
- Lack of direct head-to-head RCTs against standard antidiabetic drugs
- Heterogeneity in formulations, dosages, and application routes
- Short study duration (mostly < 12 weeks); lack of long-term data
- Low standardization of extracts (variability of active ingredient content)
- Lack of long-term safety data for combined use with standard antidiabetics
- For many terpenes (menthol, anethole, geraniol, citronellol), only preclinical evidence is available
Clinical recommendations
Based on the available evidence, the following adjuvant strategies can be considered:
- Cinnamon supplementation (0.04–0.11 oz/day Ceylon cinnamon): Adjuvant to metformin in mild hyperglycemia or prediabetes
- Ginger supplementation (2–3 g/day): Adjuvant to DPP-4 inhibitors (synergistic GLP-1 mechanism) or metformin
- Curcumin supplementation (500–1500 mg/day, bioavailable formulation): Adjuvant in T2DM with dyslipidemia, neuroinflammation, or cardiovascular risk
- Black cumin seed oil (1–3 g/day Nigella sativa): Adjuvant for T2DM with oxidative stress and beta-cell dysfunction
- Beta-Caryophyllene: Adjuvant for T2DM with a neuroinflammatory component (e.g., diabetic neuropathy)
Important notes: All essential oils should only be used as an adjunct to, not as a substitute for, prescribed antidiabetic medications. Interactions with drugs metabolized by CYP3A4/CYP2C9 should be considered. Medical advice is required.
credentials
International Diabetes Federation. (2021). IDF Diabetes Atlas, 10th edition. Brussels, Belgium. https://www.diabetesatlas.org
[D2] DeFronzo RA, Ferrannini E, Groop L, et al. (2015). Type 2 diabetes mellitus. Nature Reviews Disease Primers, 1, 15019. https://doi.org/10.1038/nrdp.2015.19
Gregg EW, Sattar N, Ali MK. (2016). The changing face of diabetes complications. The Lancet Diabetes & Endocrinology, 4(6), 537–547. https://doi.org/10.1016/S2213-8587(16)30010-9
American Diabetes Association. (2024). Standards of Medical Care in Diabetes – 2024. *Diabetes Care*, *47*(Suppl 1), S1–S321. https://doi.org/10.2337/dc24-SINT
Khunti K, Wolden ML, Thorsted BL, et al. (2013). Clinical inertia in people with type 2 diabetes: A retrospective cohort study of more than 80,000 people. Diabetes Care, 36(11), 3411–3417. https://doi.org/10.2337/dc13-0331
[D6] Fonseca ECM, Ferreira LR, Figueiredo PLB, et al. (2023). Antidepressant Effects of Essential Oils: A Review of the Past Decade (2012–2022) and Molecular Docking Study of Their Major Chemical Components. International Journal of Molecular Sciences, 24(11), 9244. https://doi.org/10.3390/ijms24119244
Saltiel AR, Kahn CR. (2001). Insulin signalling and the regulation of glucose and lipid metabolism. Nature, 414(6865), 799–806. https://doi.org/10.1038/414799a
Hardie DG, Ross FA, Hawley SA. (2012). AMPK: a nutrient and energy sensor that maintains energy homeostasis. Nature Reviews Molecular Cell Biology, 13(4), 251–262. https://doi.org/10.1038/nrm3311
Hotamisligil GS. (2006). Inflammation and metabolic disorders. Nature, 444(7121), 860–867. https://doi.org/10.1038/nature05485
Drucker DJ, Nauck MA. (2006). The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. The Lancet, 368(9548), 1696–1705. https://doi.org/10.1016/S0140-6736(06)69705-5
[D11] Zinman B, Wanner C, Lachin JM, et al. (2015). Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. New England Journal of Medicine, 373(22), 2117–2128. https://doi.org/10.1056/NEJMoa1504720
Deacon CF. (2011). Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes: a comparative review. Diabetes, Obesity and Metabolism, 13(1), 7–18. https://doi.org/10.1111/j.1463-1326.2010.01306.x
Sola D, Rossi L, Schianca GPC, et al. (2015). Sulfonylureas and their use in clinical practice. Archives of Medical Science, 11(4), 840–848. https://doi.org/10.5114/aoms.2015.53304
[D14] Nesto RW, Bell D, Bonow RO, et al. (2003). Thiazolidinedione use, fluid retention, and congestive heart failure: A consensus statement from the American Heart Association and American Diabetes Association. *Diabetes Care*, 26(10), 2941–2948. https://doi.org/10.2337/diacare.26.10.2941
[D15] Holman RR, Cull CA, Turner RC. (1999). A randomized double-blind trial of acarbose in type 2 diabetes shows improved glycemic control over 3 years. Diabetes Care, 22(6), 960–964. https://doi.org/10.2337/diacare.22.6.960
Herz RS. (2009). Aromatherapy facts and fictions: a scientific analysis of olfactory effects on mood, physiology and behavior. International Journal of Neuroscience, 119(2), 263–290. https://doi.org/10.1080/00207450802333953
[D17] Ramos GS, Valim ACSM, Brito MVC, et al. (2025). Nose-to-Brain Delivery System for Incorporating Monoterpenes with Anti-Depressant Potential. Current Neuropharmacology. https://doi.org/10.2174/011570159X380176251215113303
[D18] Hariri M, Ghiasvand R. (2016). Cinnamon and chronic diseases. Advances in Experimental Medicine and Biology, 929, 1–24. https://doi.org/10.1007/978-3-319-41342-6_1
[D19] Ranasinghe P, Pigera S, Premakumara GAS, et al. (2013). Medicinal properties of ‘true’ cinnamon (Cinnamomum zeylanicum): a systematic review. BMC Complementary and Alternative Medicine, 13, 275. https://doi.org/10.1186/1472-6882-13-275
[D20] Davis PA, Yokoyama W. (2011). Cinnamon intake lowers fasting blood glucose: meta-analysis. Journal of Medicinal Food, 14(9), 884–889. https://doi.org/10.1089/JMF.2010.0180
[D21] Hasanzadeh A, Ansari M, Davoodvandi A, et al. (2025). Efficacy and Safety of Cinnamomum zeylanicum (Ceylon cinnamon) for diabetes mellitus: a randomized, double blind, placebo-controlled clinical trial. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. https://doi.org/10.1016/j.dsx.2025.103357
[D22] Samad MB, Mohsin MNAB, Razu BA, et al. (2017). [6]-Gingerol, from Zingiber officinale, potentiates the GLP-1 mediated glucose-stimulated insulin secretion pathway in pancreatic β-cells and increases RAB8/RAB10-regulated membrane presentation of GLUT4 transporters in skeletal muscle to improve hyperglycemia in Lepr db/db type 2 diabetic mice. BMC Complementary and Alternative Medicine, 17(1), 395. https://doi.org/10.1186/S12906-017-1903-0
Daily JW, Yang M, Kim DS, Park S. (2015). Efficacy of ginger for treating Type 2 diabetes: A systematic review and meta-analysis of randomized clinical trials. Journal of Ethnic Foods, 2(1), 36–43. https://doi.org/10.1016/J.JEF.2015.02.007
Zhu J, Chen H, Song Z, et al. (2018). Effects of Ginger (Zingiber officinale Roscoe) on Type 2 Diabetes Mellitus and Components of the Metabolic Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evidence-Based Complementary and Alternative Medicine, 2018, 5692962. https://doi.org/10.1155/2018/5692962
[D25] Panahi Y, Hosseini MS, Khalili N, et al. (2015). Antioxidant and anti-inflammatory effects of curcuminoid-piperine combination in subjects with metabolic syndrome: A randomized controlled trial and an updated meta-analysis. Clinical Nutrition, 34(6), 1101–1108. https://doi.org/10.1016/j.clnu.2014.12.019
Zhang T, He Q, Liu Y, et al. (2021). Efficacy and Safety of Curcumin Supplement on Improvement of Insulin Resistance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evidence-Based Complementary and Alternative Medicine, 2021, 4471944. https://doi.org/10.1155/2021/4471944
[D27] Hosseini SA, Morvaridzadeh M, Masoudi N, et al. (2024). Curcumin extract improves beta cell functions in obese patients with type 2 diabetes: a randomized controlled trial. Nutrition Journal, 23(1), 112. https://doi.org/10.1186/s12937-024-01022-3
[D28] Mohammadi M, Ramezani-Jolfaie N, Lorzadeh E, et al. (2025). Curcumin supplementation improves the clinical outcomes of patients with diabetes and atherosclerotic cardiovascular risk. Scientific Reports, 15, 11234. https://doi.org/10.1038/s41598-025-09783-5
Hadi S, Daryabeygi-Khotbehsara R, Mirmiran P, et al. (2021). Effect of Nigella sativa oil on blood glucose in people with type 2 diabetes mellitus: A systematic review and meta-analysis. Complementary Therapies in Medicine, 56, 102592. https://doi.org/10.1016/j.ctim.2020.102592
Heshmati J, Namazi N. (2015). Effects of black seed (Nigella sativa) on metabolic parameters in diabetes mellitus: A systematic review. Complementary Therapies in Medicine, 23(2), 275–282. https://doi.org/10.1016/j.ctim.2015.01.013
Salehi B, Mishra AP, Shukla I, et al. (2018). Thymol, thyme, and other plant sources: Health and potential uses. Phytotherapy Research, 32(9), 1688–1706. https://doi.org/10.1002/ptr.6109
Cortés-Rojas DF, de Souza CRF, Oliveira WP. (2014). Clove (Syzygium aromaticum): a precious spice. Asian Pacific Journal of Tropical Biomedicine, 4(2), 90–96. https://doi.org/10.1016/S2221-1691(14)60215-X
[D33] Nagulapalli Venkata KC, Swaroop A, Bagchi D, Bishayee A. (2017). A small plant with big benefits: Fenugreek (Trigonella foenum-graecum Linn.) for disease prevention and health promotion. Molecular Nutrition & Food Research, 61(6). https://doi.org/10.1002/mnfr.201600950
Mohamad Shahi M, Haidari F, Shiri MR, et al. (2024). Therapeutic effect of fenugreek supplementation on type 2 diabetes mellitus: A systematic review and meta-analysis of clinical trials. Heliyon, 10(17), e36649. https://doi.org/10.1016/j.heliyon.2024.e36649
[D35] Navarra M, Mannucci C, Delbò M, Calapai G. (2015). Citrus bergamia essential oil: from basic research to clinical application. Frontiers in Pharmacology, 6, 36. https://doi.org/10.3389/fphar.2015.00036
McKay DL, Blumberg JB. (2006). A review of the bioactivity and potential health benefits of peppermint tea (Mentha piperita L.). Phytotherapy Research, 20(8), 619–633. https://doi.org/10.1002/ptr.1936
Mahmoud MF, Al Ali N, Mostafa IT, et al. (2022). Coriander Oil Reverses Dexamethasone-Induced Insulin Resistance in Rats. Antioxidants, 11(3), 441. https://doi.org/10.3390/antiox11030441
Rather MA, Dar BA, Sofi SN, et al. (2016). Foeniculum vulgare: A comprehensive review of its traditional use, phytochemistry, pharmacology, and safety. Arabian Journal of Chemistry, 9(Suppl 2), S1574–S1583. https://doi.org/10.1016/j.arabjc.2012.04.011
[D39] Andrade JM, Faustino C, Garcia C, et al. (2018). *Rosmarinus officinalis* L.: an update review of its phytochemistry and biological activity. *Future Science OA*, 4(4), FSO283. https://doi.org/10.4155/fsoa-2017-0124
[D40] Mani V, Badrachalam R, Shanmugam SN, et al. (2021). Effect of β-Caryophyllene on Insulin Resistance in Skeletal Muscle of High Fat Diet and Fructose-Induced Type-2 Diabetic Rats. Bioinformation, 17(7), 741–748. https://doi.org/10.6026/97320630017741
Juergens UR, Engelen T, Racké K, et al. (2004). Inhibitory activity of 1,8-cineol (eucalyptol) on cytokine production in cultured human lymphocytes and monocytes. Pulmonary Pharmacology & Therapeutics, 17(5), 281–287. https://doi.org/10.1016/j.pupt.2004.06.002
[D42] Galal RM, Shebl AM, Abdelrahman MA, et al. (2025). In silico and in vivo study: chamazulene and/or cinnamic acid modulate IRS2/GLUT4, HNF4α, GLUT2, redox system, DNA damage, and lipid profile. Future Journal of Pharmaceutical Sciences, 11, 27. https://doi.org/10.1186/s43094-025-00880-w
Lo HY, Ho TY, Li CC, et al. (2013). A novel insulin receptor-binding protein from Momordica charantia enhances glucose uptake and glucose transporter 4 translocation in 3T3-L1 adipocytes. Journal of Agricultural and Food Chemistry, 61(9), 2461–2468. https://doi.org/10.1021/jf304430y
Wang Y, Liu G, Chen M, et al. (2022). Ginsenoside F4 Alleviates Skeletal Muscle Insulin Resistance by Regulating PTP1B in Type II Diabetes Mellitus. Journal of Agricultural and Food Chemistry, 71(4), 1912–1922. https://doi.org/10.1021/acs.jafc.3c01262
[D45] Akhtar N, Jafri L, Green BD, et al. (2018). A Multi-Mode Bioactive Agent Isolated From Ficus microcarpa L. Fill. With Therapeutic Potential for Type 2 Diabetes Mellitus. Frontiers in Pharmacology, 9, 1376. https://doi.org/10.3389/FPHAR.2018.01376
Kaur R, Bhardwaj A, Gupta S. (2022). Sandalwood essential oil: A review of its pharmacological properties and therapeutic uses. Natural Product Research, 36(6), 1424–1445. https://doi.org/10.1080/14786419.2021.1923765
[D47] Siddiqui MZ. (2011). Boswellia serrata, a potential antiinflammatory agent: an overview. Indian Journal of Pharmaceutical Sciences, 73(3), 255–261. https://doi.org/10.4103/0250-474X.93507
Hongratanaworakit T, Buchbauer G. (2004). Evaluation of the harmonizing effect of ylang-ylang oil on humans after inhalation. Planta Medica, 70(7), 632–636. https://doi.org/10.1055/s-2004-827186
Kennedy DO, Little W, Scholey AB. (2004). Attenuation of laboratory-induced stress in humans after acute administration of Melissa officinalis (Lemon Balm). Psychosomatic Medicine, 66(4), 607–613. https://doi.org/10.1097/01.psy.0000132877.72833.71
Kwon H, Cho JH, Kim YJ, et al. (2022). Phytochemicals in Ocimum basilicum: A review of their pharmacological properties and therapeutic applications. Journal of Ethnopharmacology, 293, 115304. https://doi.org/10.1016/j.jep.2022.115304
Glossary
1,8-Cineole
Main active ingredient of eucalyptus/rosemary oil; anti-inflammatory, alpha-glucosidase inhibition
4-Hydroxyisoleucine
Active ingredient from fenugreek; glucose-dependent insulin secretion
5-HT1A
Serotonin-1A receptor – relevant for stress hyperglycemia
Akt/PKB
Protein kinase B – central kinase in the insulin signaling pathway; phosphorylates GLUT4 vesicle proteins
Alpha-Glucosidase
Intestinal enzyme for carbohydrate splitting; target of acarbose and several terpenes
AMPK
AMP-activated protein kinase – cellular energy sensor; main target of metformin
Boswellic acid
Active ingredient from frankincense; 5-lipoxygenase and NF-κB inhibition
CaMKKβ
Calmodulin-dependent protein kinase kinase beta – activates AMPK upstream
Carvacrol
Monoterpenes from oregano/thyme; PPARγ, alpha-glucosidase inhibition
Cat
Catalase – antioxidant enzyme; breaks down H₂O₂
CB2
Cannabinoid receptor type 2 – G-protein coupled receptor; anti-neuroinflammatory
Cinnamaldehyde
Main active ingredient of cinnamon oil (60-80 %); AMPK activator, GLUT4 inducer
Curcumin
Main active ingredient of turmeric (3–5 %); PPARγ, NF-κB, AMPK
CYP2C9
Cytochrome P450 2C9 – metabolizes sulfonylureas and some terpenes
CYP3A4
Cytochrome P450 3A4 – the most important metabolizing enzyme for terpenes and many drugs
DPP-4
Dipeptidylpeptidase-4 – Enzyme that breaks down GLP-1; target of gliptins
Eugenol
Phenylpropanoids from clove (70–90 %); Alpha-glucosidase inhibition, insulin secretion
G6Pase
Glucose-6-phosphatase – final enzyme of hepatic glucose production
Gingerol
Main active ingredient of ginger oil; GLP-1 potentiation and GLUT4 induction via Rab8/Rab10
GLP-1
Glucagon-like Peptide-1 – Incretin Hormone; stimulates glucose-dependent insulin secretion
GLUT4
Glucose transporter type 4 – insulin-dependent glucose transporter in muscle and adipose tissue
GTP
Glutathione peroxidase – antioxidant enzyme; reduces lipid peroxides
Glutathione
Glutathione – the most important intracellular antioxidant
HbA1c
Glycated Hemoglobin – Long-term Blood Sugar Marker (3-Month Average)
Homeostatic Model Assessment of Insulin Resistance (HOMA-IR)
Homeostatic Model Assessment of Insulin Resistance — Measure of Insulin Resistance
IR
Insulin receptor – Tyrosine kinase receptor; activates IRS-1/2 → PI3K → Akt → GLUT4
IRS-1/2
Insulin receptor substrate 1/2 – Adapter protein in the insulin signaling pathway
KATP
ATP-sensitive potassium channel – in beta cells; target of sulfonylureas
Limonene
Monoterpenes from citrus fruits/bergamot; antioxidant, insulin-sensitizing
Linalool
Monoterpenes from coriander/lavender; GABA-A, anxiolytic (stress hyperglycemia)
LKB1
Liver Kinase B1 – upstream kinase of AMPK
mTORC1
Mechanistic Target of Rapamycin Complex 1 – Growth/Metabolism Regulator; inhibited by AMPK
NF-κB
Nuclear Factor kappa B – Transcription factor; Master regulator of neuroinflammation
Nrf2
Nuclear factor erythroid 2-related factor 2 – Transcription factor; Master regulator of the antioxidant response
PEPCK
Phosphoenolpyruvate Carboxykinase – Key Enzyme of Gluconeogenesis in the Liver
PI3K
Phosphoinositide 3-Kinase – Key Enzyme in the Insulin Signaling Pathway
PPARγ
Peroxisome proliferator-activated receptor gamma – transcription factor; target of glitazones
PTP1B
Protein-Tyrosine Phosphatase 1B – dephosphorylates insulin receptor; inhibits insulin signaling pathway
Rab8/Rab10
Rab GTPases - Regulate GLUT4 Vesicle Exocytosis in Skeletal Muscle
ROS
Reactive Oxygen Species - Oxidative Stress Molecules
SERT
Serotonin Transporter (Reference from Depression Report)
SGLT2
Sodium-glucose cotransporter 2 – renal glucose transporter; target of gliflozins
SOD
Superoxide dismutase – antioxidant enzyme; protects against superoxide radicals
Type 2 diabetes mellitus
Type 2 diabetes mellitus – the most common form of diabetes (>90 % of all cases)
Thymoquinone
Main active ingredient of black seed oil (20-48 %); AMPK, Nrf2, beta-cell protection
trans-Anethole
Main active ingredient of fennel oil (50–80 %); Alpha-glucosidase inhibition
TRPM8
Transient Receptor Potential Melastatin 8 – Cold receptor; activated by menthol
β-Caryophyllene
Sesquiterpene; CB2 agonist; GLUT4, NF-κB inhibition